Program Report: Health Economics, 2015
The NBER Program in Health Economics focuses on the determinants and consequences of differences in health outcomes. Program members have continued their long-standing interests in such basic determinants of health as substance use, obesity, and formal schooling, but a substantial number have also diversified their portfolios to include the effects of the business cycle, pollution, and overseas military deployment on health outcomes. During the five-year period covered by this report (2010-14), researchers in the program issued 530 working papers, a 36 percent increase relative to the previous five years.
I begin this report by describing research on these new topics, and then turn to those in areas in which the program has a longer history. Given the many working papers that have appeared in the period covered by my report, I can summarize only a small number of them.
The Great Recession and Health
Studies conducted by Christopher Ruhm and others prior to the Great Recession tended to find that health improved during a recession. In a 1996 study, Ruhm pointed to such contributing factors as increases in the amount of time available to exercise, cook at home, and schedule physician visits due to unemployment; less income to purchase cigarettes, alcohol, and junk food; reductions in fatal motor vehicle accidents due to declines in driving; less job-related stress; reductions in pollution associated with lower levels of industrial activity, and expansions in health insurance coverage as low-wage workers who lose their jobs and lack employer-provided health insurance become eligible for Medicaid.1 He found that a 1 percentage point rise in unemployment led to a 0.5 percent decline in the death rate. Based on these results and similar ones in other studies, Mark L. Egan, Casey B. Mulligan, and Tomas J. Philipson argue that since gross domestic product excludes the value of leisure and the value of health, it overstates the severity of recessions.2
A much less rosy picture emerges from research that includes the Great Recession. Using more recent data than that contained in his 1996 study, Ruhm finds that total mortality has shifted over time from being strongly procyclical to being unrelated to macroeconomic conditions.3 This reflects changes in the behavior of specific causes of death. Fatalities due to cardiovascular disease and motor vehicle accidents continue to be procyclical, while deaths due to cancer and accidental poisonings have become countercyclical. The changing effect of macroeconomic conditions on cancer deaths may be due to the increasing protective effectiveness of financial resources, which can be used to fund sophisticated and expensive treatment that has become available in recent years. The behavior of accidental poisoning deaths may have occurred because declines in mental health during economic downturns are increasingly associated with the use of prescribed or illicitly obtained medications that carry risks of fatal overdoses.
Gregory Colman and Dhaval Dave present results that buttress Ruhm's findings.4 They show that while becoming unemployed is associated with a small increase in leisure-time exercise, there is a substantial decline in total physical activity. They attribute this to a disproportionate loss of jobs in manual labor, such as construction, during the Great Recession. Hence, even if unemployed people exercised more, they were not as physically active as they had been at work. The upshot was that body weight increased. This may result in long-term reductions in health, since weight gains will not necessarily be reversed once employment is regained. Moreover, due to the concentration of low-educated workers in manual jobs, the recent recession may have exacerbated health differentials between high and low socioeconomic status groups.
Janet Currie and Erdal Tekin present evidence that the housing crisis that accompanied the Great Recession led to worse health outcomes.5 They find that an increase in the number of housing foreclosures was associated with increases in medical visits for mental health (anxiety and suicide attempts), for preventable conditions (such as hypertension), and for a broad array of physical complaints that are plausibly stress-related. They also find larger effects for African-Americans and Hispanics than for whites, which is consistent with the perception that minorities were hit particularly hard.
All of the studies just mentioned deal with the United States. Tinna Laufey Ásgeirsdóttir, Hope Corman, Kelly Noonan, Þórhildur Ólafsdóttir, and Nancy E. Reichman show that the health effects of the Great Recession in Iceland may have differed from those in the United States.6 They find that the recession led to reductions in all health-compromising behaviors and that it led to reductions in certain health-promoting behaviors but increases in others. Many of these effects were due to the reduction of Iceland's real exchange rate, which increased the real prices of tobacco, alcohol, and fruits - all of which are primarily imported.
Not all the health effects experienced by U.S. citizens during the Great Recession were unfavorable. For example, Sara Markowitz, Erik Nesson, and Joshua Robinson report that reductions in labor market activity were associated with a reduced incidence of flu.7 Jason M. Lindo, Jessamyn Schaller, and Benjamin Hansen find that female layoffs reduced child abuse, while male layoffs increased it.8 Given the somewhat conflicting evidence, I suspect that program members will continue to pursue research on the effects of recessions on health for a long time.
Pollution and Health
Reductions in health have well-established negative effects on worker productivity. Tom Chang, Joshua S. Graff Zivin, Tal Gross, and Matthew J. Neidell capitalize on this relationship to study one of the effects of outdoor air pollution: its impact on the productivity and health of indoor workers at a pear-packing factory.9 They focus on fine particulate matter (PM 2.5), a harmful pollutant that easily penetrates indoor settings. They find that an increase in PM 2.5 outdoors leads to a statistically and economically significant decrease in packing speeds inside the factory, with effects arising at levels well below current air quality standards. In contrast, they find little effect of pollutants that do not travel indoors, such as ozone.
In a related study, Graff Zivin and Neidell exploit a novel panel dataset of daily farm worker output as recorded under piece-rate contracts merged with data on environmental conditions to relate the plausibly exogenous daily variations in ozone with worker productivity.10 They find robust evidence that ozone levels well below federal air quality standards have a significant impact on productivity. In particular, a 10 parts per billion decrease in ozone concentrations increases worker productivity by 4.2 percent.
Turning to the direct effects of pollution on health, Emmanuelle Lavaine and Neidell examine the effect of energy production on newborn health using a 2010 strike that affected oil refineries in France as a natural experiment.11 They show that significant reduction in sulfur dioxide (SO2) concentrations caused by the reduction in refining increased birth weight and gestational age of newborns, particularly for those exposed to the strike during the third trimester of pregnancy. Currie, Graff Zivin, Jamie Mullins, and Neidell summarize a good deal of evidence that points to a positive effect of birth weight on such adult outcomes as earnings.12 Based on that evidence, back-of-the-envelope calculations made by Lavaine and Neidell suggest that a 1 unit decline in SO2 leads to a 196 million euro increase in lifetime earnings per birth cohort.
In another study dealing with infant health outcomes, Resul Cesur, Tekin, and Aydogan Ulker explore the impact of the widespread adoption of natural gas - a relatively clean, abundant, and highly efficient source of energy - on infant mortality in Turkey.13 They report that a 1 percentage point increase in the rate of subscriptions to natural gas services would cause the infant mortality rate to decline by approximately 4 percent. This would translate into 357 infant lives saved in 2011 alone.
Graff Zivin and Neidell emphasize that avoidance behavior is an important component for understanding the difference between the biological and behavioral effects of pollution and for proper welfare computations.14 That is, the total cost imposed on society by pollution consists of the monetary value of the health reductions and the cost of resources employed to reduce or avoid increases in morbidity and mortality. In the case of avoidance behavior generated by poor water quality, Graff Zivin, Neidell, and Wolfram Schlenker estimate that U.S. consumers spent roughly $60 million on bottled water in 2005 specifically to avoid health hazards posed by drinking water violations.15
Health of Returning Veterans
Ryan Edwards examines the socioeconomic well-being and health of veterans who were deployed overseas in Iraq or Afghanistan.16 Deployment includes service in a combat or war zone, exposure to casualties, or both. He finds that the impacts on current socioeconomic well-being may be relatively small, but the effects on self-reported health are negative and substantial. His results are consistent with a veterans’ compensation system that replaces lost earnings but does not necessarily compensate for other harms associated with combat exposure, such as mental health trauma.
Cesur, Joseph J. Sabia, and Tekin examine the effects of recent deployments by focusing on a different health indicator than the one used by Edwards: adverse mental health.17 Their use of longitudinal data allows them to condition on mental health prior to deployment and a number of other potential confounders. They argue persuasively that deployment assignments are exogenous, not based on individual soldiers' characteristics such as perceived bravery, mental toughness, or family circumstances, but rather on the operational needs of the armed forces. They find that soldiers deployed to combat zones where they engage in frequent firefights or witness allied or civilian deaths are at substantially increased risk of suicidal ideation and post-traumatic stress disorder (PTSD). Their estimates imply lower-bound health care costs of $1.5 to $2.7 billion for combat-induced PTSD.
Unhealthy Behaviors
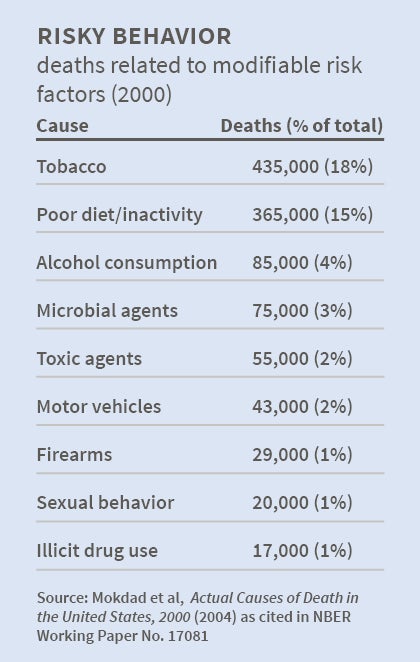
Tobacco use, obesity resulting from overeating and lack of exercise, excessive alcohol consumption, and illegal drug use rank first, second, third, and ninth, respectively, as the leading causes of premature mortality in the United States and most other countries in the developed world. These behaviors also have substantial effects on morbidity and are associated with such other negative outcomes as child abuse, spouse abuse, fires, crime, and risky sexual encounters. John Cawley and Ruhm present an overview of economic approaches to these behaviors that have been developed by program members and other researchers.18 They also summarize empirical evidence concerning the effects of prices, taxes, and government-enacted regulations on unhealthy behaviors from studies conducted prior to 2010. Since consumption of the goods at issue in the present has harmful effects on health in the future, the rate at which people discount the future consequences of their current actions is an important determinant of the consumption of these substances. The greater the rate of time preference for the present, the more likely it is that a person will consume goods that are harmful to his or her health.
Cawley and Ruhm point out that the time discount factor can vary among consumption choices. For example, individuals may heavily discount the harmful effects of eating junk food, while they give much more weight to the harmful effects of cigarette smoking. Henry Saffer pursues this insight by employing a novel empirical approach to create a single measure of self-regulation (a concept that is closely related to time preference) that can vary across domains.19 This approach allows for the study of how self-regulation is correlated across different health choices. The results show that there is a high correlation in self-regulation for smoking, drinking, drug use, and crime. However, self-regulation for body mass index (BMI, defined as weight in kilograms divided by height in meters squared) and for obesity (BMI equal to or greater than 30) is different than self-regulation for the other outcomes. The results also show that self-regulation has a significant negative effect on all choices.
Tobacco
Program members have continued to collect evidence on the relative effectiveness of tobacco excise tax hikes on the use of tobacco products and related outcomes. Jidong Huang and Frank J. Chaloupka IV examine the impact of the 2009 federal tobacco excise tax increase on the use of cigarettes and smokeless tobacco products among youths ages 14–18.20 The results of this analysis show that this tax increase had a substantial short-term impact. The percentage of students who reported smoking in the past 30 days dropped between 10 and 13 percent, and the percentage of students who reported using smokeless tobacco products dropped between 16 and 24 percent.
The long-term projected number of youths prevented from smoking or using smokeless tobacco that resulted from the 2009 federal tax increase could be much larger, since the higher tobacco prices would deter more and more children from initiating smoking and smokeless tobacco use over time.
Markowitz considers the effects of cigarette excise tax hikes on fires, one of the negative consequences of smoking.21 She finds that increases in state excise tax rates on cigarettes are associated with fewer fires. In another study dealing with a negative consequence of smoking, Markowitz, E. Kathleen Adams, Patricia M. Dietz, Viji Kannan, and Van Tong report that higher cigarette taxes are associated with small increases in birth weight and gestational weeks for teenage mothers.22 The mechanism here is that maternal smoking during pregnancy leads to poor birth outcomes.
Kevin Callison and Robert Kaestner question the consensus that raising tobacco taxes reduces cigarette consumption across the board.23 They find that for adults the association between state tax hikes and either smoking participation or smoking intensity is negative, small, and not statistically significant. These results do not conflict with those that have been observed for teenagers and young adults.
Turning to other determinants of tobacco use, Dave and Saffer provide the first estimates of the effects of magazine advertising on smokeless tobacco (ST) use.24 While the prevalence of ST use is low relative to smoking, the distribution of use is highly skewed, with consumption concentrated among certain segments of the population, such as rural residents, males, whites, and low-educated individuals. Furthermore, there is suggestive evidence that use has trended upwards recently for groups that traditionally have been at low risk of using ST. Dave and Saffer's focus on magazine advertising is significant given that tobacco manufacturers have been banned from using other conventional media for many years. They find consistent and robust evidence that exposure to ST ads in magazines raises ST use, especially among males. They also present suggestive evidence that both ST taxes and cigarette taxes reduce ST use, indicating contemporaneous complementarity between these tobacco products. Since ST use is less harmful than cigarette smoking, effects from this study inform the debate on the cost and benefits of ST use and its potential to be a tool in overall reduction of tobacco-related harm.
Restrictions on smoking in public places are the most noticeable non-price tobacco control measures worldwide, yet surprisingly little is known about their effects on exposure to environmental tobacco smoke (ETS), commonly termed second-hand smoke. Using data for Canada, Christopher Carpenter, Sabina Postolek, and Casey Warman found these laws had no effects on smoking but induced large and statistically significant reductions in ETS exposure in public places, especially in bars and restaurants.25 They did not find significant evidence of ETS displacement to private homes. Their results indicate a potential for substantial health improvements from banning smoking in public places.
Alcohol
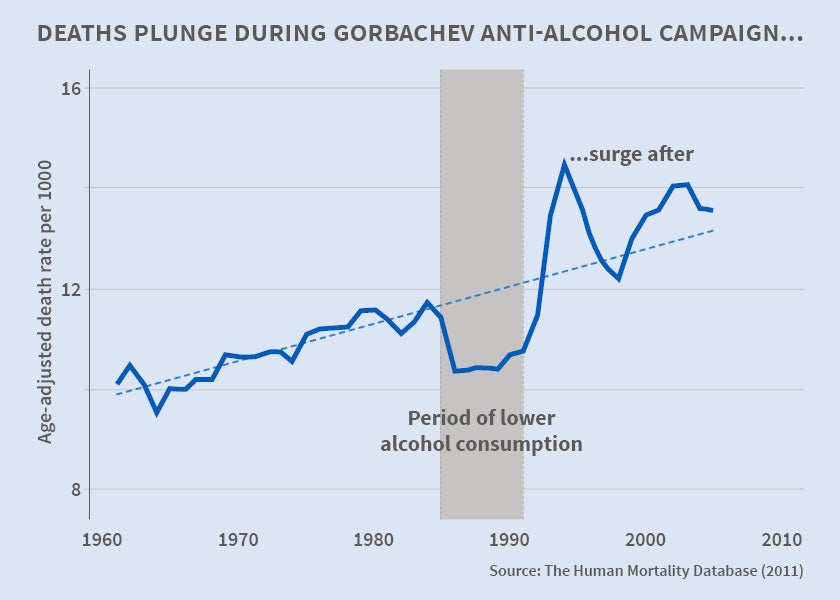
Program members have focused on the effects of alcohol misuse and overuse and on the effects of regulations of these behaviors on motor vehicle accident mortality, other causes of mortality, and crime. Jay Bhattacharya, Christina Gathmann, and Grant Miller show that the end of the 1985-88 Gorbachev Anti-Alcohol Campaign, and not Russia's transition to capitalism, was responsible for a large part of the 40 percent surge in deaths between 1990 and 1994.26 Philip J. Cook and Christine Piette Durrance report that the 1991 U.S. federal excise tax hikes on beer, wine, and distilled spirits reduced deaths due to crashes and other accidents by approximately 5 percent, or almost 7,000 lives, in that year.27 In addition, the tax increases led to reductions in violent crime and property crime. Hansen finds that increasing punishments and sanctions for repeat drunk-driving offenders and making penalties stiffer the higher the offender's blood-alcohol content (BAC) are much more effective deterrents than policies to lower the BAC level required for conviction.28 Hope Corman and Naci H. Mocan employ monthly data over 19 years for New York City and after correcting for policy endogeneity find that alcohol consumption is positively related to assault, rape, and larceny crimes but not to murder, robbery, burglary, or motor vehicle theft.29
Illegal Drugs
As a result of the 2012 and 2014 elections, four U.S. states - Alaska, Oregon, Colorado, and Washington - legalized the use of marijuana for recreational purposes. Moreover, laws enacted by an additional 19 states since 1996 have legalized marijuana use for medical purposes. Spurred by these developments, program members have investigated the impacts of these laws on marijuana use, alcohol use, and motor vehicle accident mortality. The laws reduce the price of marijuana and should lead to an increase in its use. They may reduce the use of alcohol if that substance and marijuana are substitutes, while they may increase the use of alcohol if the two substances are complements. If alcohol and marijuana are substitutes, they also have the potential to reduce motor vehicle accident mortality, because simulator and driver-course studies show that impairments due to alcohol increase the risk of a collision, while impairments due to the use of marijuana do not. Drivers under the influence of marijuana reduce their speed, avoid risky maneuvers, and increase "following distances." Drivers under the influence of alcohol behave in the opposite manner.30
Program members have taken a 2013 study by D. Mark Anderson, Hansen, and Daniel I. Rees, completed before Hansen became a Faculty Research Fellow in the Health Economics Program, as the point of departure for their research.31 Using data from the period from 1990 through 2010, their study finds that use of marijuana rose and alcohol-related traffic fatalities fell by 13 percent in the 13 states that enacted medical marijuana laws during the sample period. At the same time consumption of alcohol, including binge drinking (consumption of five or more drinks of alcohol in a row for males and four or more drinks in a row for females) fell. These findings, which pertain to adults, are consistent with the notion that alcohol and marijuana are substitutes; reductions in the price of marijuana lead to increases in its use and reductions in the use of alcohol. The authors found no evidence that marijuana use by youths increased. The same authors in a subsequent paper using a larger dataset again find no effect on use by teenagers.32
Rosalie Liccardo Pacula, Paul Heaton, David Powell, and Eric Sevigny focus on policy differences among states that have adopted medical marijuana laws and analyze the effects of these laws on all outcomes considered in the studies just discussed.33 These dimensions include whether states require patient registry systems, whether states permit home cultivation, whether states legally allow dispensaries, and whether states make allowance for "pain" rather than only for specific medical conditions. They show that inclusion of these dimensions clouds the sharp results in the studies by Anderson, Hansen, and Rees. Pacula and her colleagues are unable to draw firm conclusions with regard to the effects of the laws on marijuana use, alcohol use, and alcohol-involved fatal crashes.
To complicate the picture even further, Heifei Wen, Jason M. Hockenberry, and Janet R. Cummings employ a dataset not used in previous studies and find that the enactment of medical marijuana laws is associated with an increase in the probability of use by youths and adults.34 Frequency of use and binge drinking increased among adults but not youths. Hopefully, these disparate findings will be better understood as data for longer periods of time become available.
Obesity
Prior research on obesity has focused on body mass index (BMI) as the primary outcome. This is understandable because it is easy to calculate BMI from data on height and weight, both of which are readily available from many social science datasets. The problem with this measure is that it has somewhat limited ability to distinguish body fat from lean body mass. Since it is body fat and not fat-free mass that is responsible for the detrimental effects of obesity, Tekin, Roy Wada, and I use a direct measure of body composition - percentage body fat (PBF, defined as body fat as a percentage of total weight) - in a study of the effects of food prices on obesity in youth ages 12 through 18.35 We obtain these measures from bioelectrical impedance analysis or dual energy x-ray absorptiometry conducted during physical examinations, and find that a 10 percent increase in the real price per calorie of food for home consumption lowers PBF by about 9 percent for males and by about 8 percent for females. We also find that an increase in the real price of fast-food restaurant food leads to a reduction in PBF, while a rise in the real price of fruits and vegetables leads to an increase in this outcome. Finally, we show that nonwhite youths are particularly sensitive to fast-food restaurant prices.
An explanation of the last result is that the "full" price of fast-food consumption consists of the money price and the monetary value of the future health consequences of that consumption. A 1 percent change in the money price results in a larger percentage change in the full price when future health costs are small than when they are large. Future costs are likely be less important to parents and youths in the poorer, less-educated families in which a substantial proportion of nonwhite youths reside because these factors are associated with higher rates of time preference for the present. Charles J. Courtemanche, Garth Heutel, and Patrick McAlvanah provide direct evidence in support or the argument just made.36 They find that the body mass index of people around the age of 45 who discount the future heavily based on survey responses is more sensitive to a general measure of the price of food than the body mass index of other consumers.
Tatiana Andreyeva, Inas Rashad Kelly, and Jennifer L. Harris focus on another important determinant of weight outcomes in children - food advertising on television.37 Their results suggest that television advertising for soft drinks and fast food leads to increased consumption of these commodities among elementary school children in the fifth grade. Exposure to 100 incremental TV ads for sugar-sweetened carbonated soft drinks was associated with a 9 percent rise in children's consumption of soft drinks. The same increase in exposure to fast-food advertising was associated with a 1 percent rise in children's consumption of fast food. There was no detectable link between advertising exposure and average body weight, but fast-food advertising was significantly associated with body mass index for overweight and obese children, revealing detectable effects for a vulnerable group.
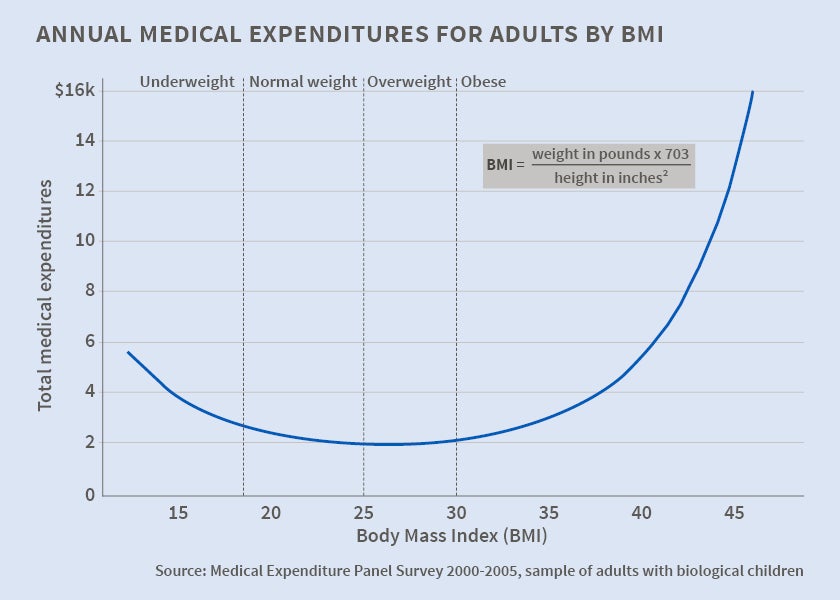
Turning to one of the important consequences of obesity, Cawley and Chad Meyerhoefer exploit genetic variation in weight as a source of variation and find that weight's impact on medical costs is approximately 4 times greater than suggested by estimates that do not control for endogeneity.38 They estimate the annual cost of treating obesity in the U.S. at $168 billion, or 16 percent of national spending on medical care. The upshot is that the previous literature has underestimated the cost effectiveness of anti-obesity interventions.
Schooling and Health
Years of formal schooling completed and health are the two most important components of the stock of human capital, and it is natural to examine complementarities between them. This task is challenging because causality may run both from more schooling to better health and from better health to more schooling. In addition there may be omitted "third variables" that cause both schooling and health to vary in the same direction. Program members have employed quasi-natural experiments, instrumental variables techniques, temporal ordering, and novel measures of third variables to study this relationship.
Ming-Jen Lin and Elaine M. Liu test the fetal origins hypothesis, namely that in utero conditions affect long-run developmental outcomes, using the 1918 influenza pandemic in Taiwan as a natural experiment.39 They find that cohorts in utero during the pandemic are shorter as children/adolescents and less educated as adults compared to other birth cohorts. They also find that they are more likely to have serious health problems including kidney disease, circulatory and respiratory problems, and diabetes in old age.
Gabriella Conti and James J. Heckman show that pre-school interventions in low-income populations of U.S. children have positive effects on a variety of measures of well-being in adulthood, including formal schooling completed and health.40 They also provide direct evidence in support of the causal effects of education on health in a British panel dataset. Using insights from psychology, they emphasize the "big five personality traits" (conscientiousness, openness, extraversion, agreeableness, and neuroticism) as hard-to-measure factors that influence both health and schooling. Controlling for these measures, cognitive ability, and health, all at age ten, they find that the positive effects of education on self-rated health at age 30, and the negative effects of this variable on smoking and obesity at that age are positively associated with cognitive ability and negatively associated with noncognitive ability.
Damon Clark and Heather Royer exploit changes in British compulsory schooling laws that generated sharp differences in educational attainment among cohorts born months apart to evaluate the causal impacts of education on adult mortality and health behaviors.41 Kasey Buckles, Andreas Hagemann, Ofer Malamud, Melinda S. Morrill, and Abigail K. Wozniak pursue a similar instrumental variable strategy but with a different instrument - college completion induced by draft avoidance behavior during the Vietnam War42 Results in the two studies are very different. Clark and Royer find no evidence that increased schooling improved health outcomes or changed health behaviors, while Buckles and colleagues find that college completion reduced cumulative mortality from 1980–2007 by almost 30 percent relative to the mean for men ages 38-49 in 1980. They also report negative effects of college completion on smoking, heavy drinking, and obesity, and a positive effect on exercise.
Health Insurance and Health
Much of the research of the program focuses on the non-medical care determinants of health and the response of those determinants to economic factors. Some investigators, however, consider the effects of medical care and its key determinant - health insurance.
Courtemanche and Daniela Zapata present evidence that the health care reform legislation enacted by Massachusetts and designed to achieve nearly universal coverage led to better overall self-assessed health.43 They also document improvements in several determinants of overall health: physical health, mental health, functional limitations, joint disorders, and body mass index. Finally, they show that the effects on overall health were strongest among those with low incomes, nonwhites, near-elderly adults, and women.
Kaestner, Cuiping Long, and G. Caleb Alexander examine whether obtaining prescription drug insurance through the Medicare Part D program affected hospital admissions, expenditures associated with those admissions, and mortality.44 They use a large, geographically diverse sample of Medicare beneficiaries and exploit the natural experiment of Medicare Part D to obtain estimates of the effect of prescription drug insurance on hospitalizations and mortality. Results indicate that obtaining prescription drug insurance through Medicare Part D was associated with an 8 percent decrease in the number of hospital admissions, a 7 percent decrease in Medicare expenditures, and a decrease in total resource use. Gaining prescription drug insurance through Medicare Part D was not, however, significantly associated with mortality.
Infant and Child Health
The program has had a longstanding interest in the determinants of infant and child health outcomes. Since unplanned pregnancies and births compromise both outcomes, reproductive behavior is one of the most important of these determinants. Three studies have examined the causal impact of women's schooling on their knowledge and use of contraception. Mabel Andalón, Jenny Williams, and I investigate this issue using information on women in Mexico.45 In order to identify the causal effect of schooling, we exploit temporal and geographic variation in the number of lower secondary schools built following the extension of compulsory education in Mexico from 6th to 9th grade in 1993. We show that raising females' schooling beyond the 6th grade increases their knowledge of contraception during their reproductive years and increases their propensity to use contraception at sexual debut. Mehmet Alper Dinçer, Neeraj Kaushal, and I adopt the same research design to construct an instrument from the 1997 increase in compulsory schooling in Turkey and obtain similar results.46 Mocan and Colin Cannonier show that the increase in women's schooling caused by expanded access to free primary education in Sierra Leone, which occurred between 2001 and 2005 and varied across areas of the country, resulted in a greater propensity to use modern contraception and to be tested for AIDS.47 Expansion of education also caused reductions in pregnancies and family size in Turkey and in desired family size in Sierra Leone. Improvements in infant health typically accompany the developments just documented.
In three studies, Theodore J. Joyce and colleagues focus on policy initiatives and regulations that impact abortion - an obvious mechanism to check unplanned births. Silvie Colman and Joyce show that Texas's Women's Right to Know Act, which went into effect in January 2004 and requires that all abortions at 16 weeks gestation or later be performed in an ambulatory surgical center, reduced the in-state late-term abortion rate for 2006 by 50 percent below its pre-Act level.48 In a second study, Colman, Thomas S. Dee, and Joyce show that parental involvement laws, which require that physicians notify or obtain consent from a parent of a minor seeking an abortion before performing the procedure, have no effects on the rates of sexually transmitted infections or measures of risky sexual behaviors.49 In a third study, Joyce, Ruoding Tan, and Yuxiu Zhang use unique data on abortions performed in New York State from 1971 to 1975 to demonstrate that women traveled hundreds of miles for a legal abortion before the Supreme Court decision in Roe v. Wade that legalized abortion in all states.50 A 100-mile increase in distance for women who live approximately 800 miles from New York was associated with a decline in abortion rates of 3 percent. They also found a positive and robust association between distance to the nearest abortion provider and teen birth rates, but less-consistent estimates for other ages. Their results suggest that even if some states lost all abortion providers due to legislative policies, the impact on aggregate birth and abortion rates would be small, as most women would travel to states with abortion services.
Turning finally to studies that consider the determinants of infant and child health, Mocan, Christian Raschke, and Bulent Unel use skill-based technology shocks as an instrument to show that an increase in weekly earnings of low-skill mothers prompts an increase in prenatal care and has a small positive effect on the birth weight and gestational age of these mothers' newborns.51 Clive Belfield and Kelly report that breastfeeding at birth raises the probability that infants will be in excellent health at nine months, and is protective against obesity at 24 and 54 months.52 Brian A. Jacob, Jens Ludwig, and Douglas L. Miller focus on mortality between the ages of one and 18 and demonstrate that children who resided in low-income families in Chicago who were offered a housing voucher to move to better neighborhoods had much lower rates of mortality than those in matched families who were not offered the voucher.53
Endnotes
C. J. Ruhm, "Are Recessions Good for Your Health?" NBER Working Paper 5570, May 1996, and the Quarterly Journal of Economics, 115(2), 2000, pp. 617-50.
M. L. Egan, C. B. Mulligan, and T. J. Philipson, "Adjusting National Accounting for Health: Is the Business Cycle Countercyclical?" NBER Working Paper 19058, May 2013.
C. J. Ruhm, "Recessions, Healthy No More?" NBER Working Paper 19287, August 2013.
G. Colman and D. M. Dave, "Unemployment and Health Behaviors Over the Business Cycle: a Longitudinal View," NBER Working Paper 20748, December 2014.
J. Currie and E. Tekin, "Is there a Link Between Foreclosure and Health?" NBER Working Paper 17310, August 2011, and the American Economic Journal: Economic Policy, 7(1), 2015, pp.63-94.
T. L. Ásgeirsdóttir, H. Corman, K. Noonan, Þ. Ólafsdóttir, and N. E. Reichman, "Are Recessions Good for Your Health Behaviors? Impacts of the Economic Crisis in Iceland," NBER Working Paper 18233, July 2012.
S. Markowitz, E. Nesson, and J. Robinson, "Are Pink Slips Better Than Flu Shots? The Effects of Employment on Influenza Rates," NBER Working Paper 15796, March 2010.
J. M. Lindo, J. Schaller, and B. Hansen, "Economic Conditions and Child Abuse," NBER Working Paper 18994, April 2013.
T. Chang, J. S. Graff Zivin, T. Gross, and M. J. Neidell, "Particulate Pollution and the Productivity of Pear Packers," NBER Working Paper 19944, February 2014.
J. S. Graff Zivin and M. J. Neidell, "The Impact of Pollution on Worker Productivity," NBER Working Paper 17004, April 2011, and the American Economic Review, 102(7), 2012, pp. 3652-73.
E. Lavaine and M. J. Neidell, "Energy Production and Health Externalities: Evidence from Oil Refinery Strikes in France," NBER Working Paper 18974, April 2013.
J. Currie, J. S. Graff Zivin, J. Mullins, and M. J. Neidell, "What Do We Know About Short and Long Term Effects of Early Life Exposure to Pollution?" NBER Working Paper 19571, October 2013, and the Annual Review of Resource Economics, 6(1), 2014, pp. 217-47.
R. Cesur, E. Tekin, and A. Ulker, "Air Pollution and Infant Mortality: Evidence from the Expansion of Natural Gas Infrastructure," NBER Working Paper 18736, January 2013.
J. S. Graff Zivin and M. Neidell, "Environment, Health, and Human Capital," NBER Working Paper 18935, April 2013.
J. S. Graff Zivin, M. Neidell, and W. Schlenker, "Water Quality Violations and Avoidance Behavior: Evidence from Bottled Water Consumption," NBER Working Paper 16695, January 2011, and the American Economic Review, 101(3), 2011, pp. 448-53.
R. D. Edwards, "Overseas Deployment, Combat Exposure, and Well-Being in the 2010 National Survey of Veterans," NBER Working Paper 18227, July 2012.
R. Cesur, J. J. Sabia, and E. Tekin, "The Psychological Costs of War: Military Combat and Mental Health," NBER Working Paper 16927, April 2011, and the Journal of Health Economics, 32(1), 2013, pp. 51-65. ↩
J. Cawley and C. Ruhm, "The Economics of Risky Health Behaviors," NBER Working Paper 17081, May 2011, and in P. P. Barros, T. McGuire, and M. Pauly, eds., Handbook of Health Economics, Volume 2, Amsterdam, The Netherlands: Elsevier, North Holland, 2012, pp. 95-199.
H. Saffer, "Self-regulation and Health," NBER Working Paper 20483, September 2014.
J. Huang and F. J. Chaloupka, IV, "The Impact of the 2009 Federal Tobacco Excise Tax Increase on Youth Tobacco Use," NBER Working Paper 18026, April 2012.
S. Markowitz, "Where There's Smoking, There's Fire: The Effects of Smoking Policies on the Incidence of Fires in the United States," NBER Working Paper 16625, December 2010.
S. Markowitz, E. Kathleen Adams, P. M. Dietz, V. Kannan, and V. Tong, "Smoking Policies and Birth Outcomes: Estimates From a New Era," NBER Working Paper 17160, June 2011.
K. Callison and R. Kaestner, "Do Higher Tobacco Taxes Reduce Adult Smoking? New Evidence of the Effect of Recent Cigarette Tax Increases on Adult Smoking," NBER Working Paper 18326, August 2012, and Economic Inquiry, 52(1), 2013, pp. 155-72.
D. M. Dave and H. Saffer, "Demand for Smokeless Tobacco: Role of Magazine Advertising," NBER Working Paper 18003, April 2012, and the Journal of Health Economics, 32(4), 2013, pp. 682-97.
C. Carpenter, S. Postolek, and C. Warman, "Public-Place Smoking Laws and Exposure to Environmental Tobacco Smoke (ETS)," NBER Working Paper 15849, March 2010, and the American Economic Journal: Economic Policy, 3(3) August, 2011, pp. 35-61.
J. Bhattacharya, C. Gathmann, and G. Miller, "The Gorbachev Anti-Alcohol Campaign and Russia's Mortality Crisis," NBER Working Paper 18589, December 2012, and the American Economic Journal: Applied Economics, 5(2), 2013, pp. 232-60.
P. J. Cook and C. Piette Durrance, "The Virtuous Tax: Lifesaving and Crime-Prevention Effects of the 1991 Federal Alcohol-Tax Increase," NBER Working Paper 17709, December 2011, and the Journal of Health Economics, 32(1), 2013, pp. 261-67.
B. Hansen, "Punishment and Deterrence: Evidence from Drunk Driving," NBER Working Paper 20243, June 2014, and the American Economic Review, 105(4), 2015, pp. 1581-1617.
H. Corman and N. H. Mocan, "Alcohol Consumption, Deterrence, and Crime in New York City," NBER Working Paper 18731, January 2013.
E. Kelly, S. Darke, and J. Ross, "A Review of Drug Use and Driving: Epidemiology, Impairment, Risk Factors, and Risk Perceptions," Drug and Alcohol Review, 23(3), 2004, pp. 319-44; R. A. Sewell, J. Poling, and M. Sofuoglu, "The Effect of CannabisCompared with Alcohol on Driving," American Journal on Addictions, 18(3), 2009, pp. 185-93.
D. M. Anderson, B. Hansen, and D. I. Rees, "Medical Marijuana Laws, Traffic Fatalities, and Alcohol Consumption," Journal of Law and Economics, 56(2), 2013, pp. 333-69.
D. M. Anderson, B. Hansen, and D. I. Rees, "Medical Marijuana Laws and Teen Marijuana Use," NBER Working Paper 20332, July 2014.
R. L. Pacula, D. Powell, P. Heaton, and E. L. Sevigny, "Assessing the Effects of Medical Marijuana Laws on Marijuana and Alcohol Use: The Devil is in the Details," NBER Working Paper 19302, August 2013.
H. Wen, J. Hockenberry, and J. R. Cummings, "The Effect of Medical Marijuana Laws on Marijuana, Alcohol, and Hard Drug Use," NBER Working Paper 20085, May 2014, and the Journal of Health Economics, forthcoming.
M. Grossman, E. Tekin, and R. Wada, "Food Prices and Body Fatness among Youths," NBER Working Paper 19143, June 2013, and Economics & Human Biology, 12(January), 2014, pp. 4-19.
C. J. Courtemanche, G. Heutel, P. McAlvanah, "Impatience, Incentives, and Obesity," NBER Working Paper 17483, October 2011, and the Economic Journal, forthcoming.
T. Andreyeva, I. R. Kelly, and J. L. Harris, "Exposure to Food Advertising On Television: Associations With Children's Fast Food and Soft Drink Consumption and Obesity," NBER Working Paper 16858, March 2011, and Economics and Human Biology, 9(3), 2011, pp. 221-33.
J. Cawley, C. Meyerhoefer, "The Medical Care Costs of Obesity: An Instrumental Variables Approach," NBER Working Paper 16467, October 2010, and the Journal of Health Economics, 31(1), 2012, pp. 219-30.
M.-J. Lin and E. M. Liu, "Does in utero Exposure to Illness Matter? The 1918 Influenza Epidemic in Taiwan as a Natural Experiment," NBER Working Paper 20166, May 2014, and the Journal of Health Economics, 37, September 2014, pp. 152-63.
G. Conti and J. J. Heckman, "The Developmental Approach to Child and Adult Health," NBER Working Paper 18664, December 2012.
D. Clark and H. Royer, "The Effect of Education on Adult Health and Mortality: Evidence from Britain," NBER Working Paper 16013, May 2010, and the American Economic Review, 106(6), 2013, pp. 2087-2120.
K. Buckles, A. Hagemann, O. Malamud, M. S. Morrill, and A. K. Wozniak, "The Effect of College Education on Health," NBER Working Paper 19222, July 2013.
C. J. Courtemanche, D. Zapata, "Does Universal Coverage Improve Health? The Massachusetts Experience," NBER Working Paper 17893, March 2012, and the Journal of Policy Analysis and Management, 33(1), 2014, pp. 36-69.
R. Kaestner, C. Long, G. C. Alexander, "Effects of Prescription Drug Insurance on Hospitalization and Mortality: Evidence from Medicare Part D," NBER Working Paper 19948, February 2014.
M. Andalón, J. Williams, and M. Grossman, "Empowering Women: The Effect of Schooling on Young Women's Knowledge and Use of Contraception," NBER Working Paper 19961, March 2014.
M. A. Dinçer, N. Kaushal, and M. Grossman, "Women's Education: Harbinger of Another Spring? Evidence from a Natural Experiment in Turkey," NBER Working Paper 19597, October 2013, and World Development, 64(December), 2014, pp. 243-58.
N. H. Mocan and C. Cannonier, "Empowering Women Through Education: Evidence from Sierra Leone," NBER Working Paper 18016, April 2012.
S. Colman and T. J. Joyce, "Regulating Abortion: Impact on Patients and Providers in Texas," NBER Working Paper 15825, March 2010, and the Journal of Policy Analysis and Management, 30(4), 2011, pp. 775-97.
S. Colman, T. S. Dee, and T. J. Joyce, "Do Parental Involvement Laws Deter Risky Teen Sex?" NBER Working Paper 18810, February 2013, and the Journal of Health Economics, 32(5), 2013, pp. 873-80.
T. J. Joyce, R. Tan, and Y. Zhang, "Back to the Future? Abortion Before & After Roe," NBER Working Paper 18338, August 2012, and as "Abortion Before and After Roe," Journal of Health Economics, 32(3), 2013, pp. 804-15.
N. Mocan, C. Raschke, and B. Unel, "The Impact of Mothers' Earnings on Health Inputs and Infant Health," NBER Working Paper 19434, September 2013.
C. R. Belfield and I. R. Kelly, "The Benefits of Breastfeeding Across the Early Years of Childhood," NBER Working Paper 16496, October 2010, and the Journal of Human Capital, 6(3), 2012, pp. 251-77.
B. A. Jacob, J. Ludwig, and D. L. Miller, "The Effects of Housing and Neighborhood Conditions on Child Mortality," NBER Working Paper 17369, August 2011, and the Journal of Health Economics, 32(1), 2013, pp. 195-206.


