Smoking Patterns and the Widening US Mortality Gap
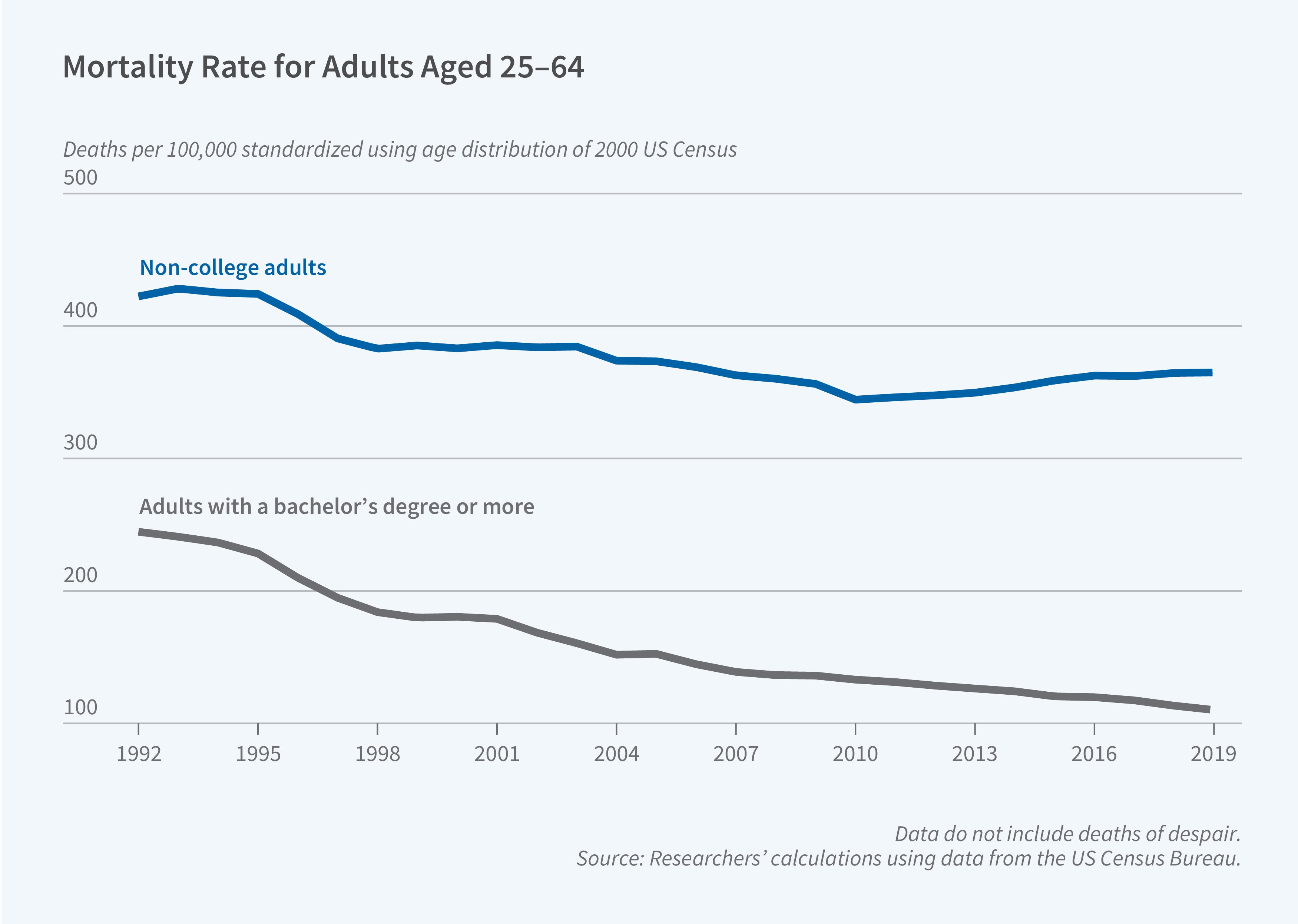
Over the past three decades, the life expectancy gap between Americans with and without college degrees widened from 2.6 years in 1992 to 6.3 years. At the same time, geographic differences in mortality have increased dramatically. Rural counties that once enjoyed lower mortality rates than urban areas now experience approximately 50 percent higher death rates. In Explaining the Widening Divides in US Midlife Mortality: Is There a Smoking Gun? (NBER Working Paper 34553), Christopher L. Foote, Ellen Meara, Jonathan S. Skinner, and Luke R. Stewart examine three coincident trends: the expanding education-mortality gradient, rising geographic inequality in death rates, and the reversal of the traditional rural health advantage.
The researchers use restricted mortality data from the National Center for Health Statistics covering 44 states from 1992 to 2019 combined with county-level population data from the National Cancer Institute's SEER program. They calculate age-adjusted mortality rates for adults aged 25–64, separating college graduates from those without four-year degrees. To assess health behaviors, they draw on individual-level data from the Behavioral Risk Factor Surveillance System, averaging smoking and obesity rates within county-education groups from 1996 to 2010.
For college graduates, mortality rates declined substantially and converged across locations. Montana's college graduate mortality rate fell from 225 per 100,000 in 1992 to 135 in 2019. New York’s fell from 337 to 120. In contrast, while average non-college mortality barely changed, spatial variation increased dramatically. New York's non-college rate fell from 521 to 385, while Montana's rose from 393 to 472.
It is well known that college graduates smoke far less often than non-college graduates, and the researchers find that smoking rates are the strongest predictor of mortality changes at the county level. A 1-standard-deviation increase in the non-college smoking rate corresponds to 53 additional deaths per 100,000 persons, and close to half of the variation in non-college mortality changes can be explained by smoking rates, initial mortality rates, and rural-urban status. When the researchers include a number of other variables in their estimating equations—such as obesity, income, employment, manufacturing share, China trade shock exposure, and state policy liberalism—smoking retains its strong effect while the impact of the other variables is attenuated. Smoking rates show minimal predictive power, however, for explaining the mortality rates of college graduates.
The link between past smoking and current mortality operates through health capital depreciation. Individuals typically begin smoking around age 18, but experience mortality effects decades later, particularly between the ages of 55 and 64. Thus, the researchers estimate that in 1992, a 10-percentage-point increase in a location’s non-college smoking rate was associated with 98 additional deaths per 100,000 nearly three decades later, in 2019. A 10-percentage-point decline in smoking over the 1992–2019 period reduced 2019 mortality by 137 per 100,000.
The researchers acknowledge that the gap between college and non-college smoking rates has been narrowing recently. How then can smoking explain a widening gap in mortality? Data from the Tobacco Use Supplement to the Current Population Survey show that in 2018–19, 76 percent of college graduates aged 55–64 had never smoked, compared to 56 percent of non-college adults—a substantial divergence from the nearly identical 41 and 43 percent rates in 1992–93. That is, the long-lasting health effects of past smoking behavior—which correlates strongly with a variety of diseases—may still be leading to the current divergence in mortality. There is some good news, which is the decline in smoking rates for younger non-college graduates; future non-college midlife mortality is expected to decline as a consequence.


