Innovative Investments in Local Jails
In research conducted in collaboration with Arkey Barnett at the University of Michigan and Meghan Beal at the National Sheriffs’ Association, we investigate the effects of innovative investments in local jails that aim to improve health and rehabilitation outcomes for incarcerated individuals and their communities. The US has one of the highest incarceration rates in the world, with nearly 2 million people detained in correctional facilities every year. While most people are held in state or federal prisons, local jails house 546,000 individuals across 3,116 facilities, the majority of whom are not convicted. Local jails serve as the front door to the criminal justice system, with more than 7.6 million admissions per year and a significant share of those released being rebooked within the same year, revealing a persistent cycle of incarceration in local jails.
At the same time, incarceration coincides with ongoing public health crises. Individuals in jail have disproportionately high rates of disease, including substance use disorder, hypertension, diabetes, and serious mental health illness. Mortality in local jails has increased over the last two decades, with suicide and substance-use-related causes accounting for a large share of in-custody deaths.
High recidivism and rising mortality in local jails reflect a common challenge: Although often viewed as short-term detention facilities, local jails profoundly shape both short- and long-run outcomes for the millions of people cycling through them and the communities to which they return. This creates a critical intervention point where rehabilitative investments can influence outcomes both within and beyond jail walls and generate outsize returns in community safety and health.
Since the 1970s, a dominant view in US criminal justice was that “nothing works,” meaning that interventions that invest in incarcerated populations had little private or social return.1 This perspective emphasizes harsh conditions as a means of deterring future criminal behavior. In contrast, an investment approach emphasizes rehabilitation through improvements in mental and physical health, education, and overall wellbeing.
Through collaboration with practitioners and leaders in the correctional system, our recent research revisits this idea and examines two distinct but complementary investments inside local jails. One study examines a top-down approach that improves healthcare services in jails through external accreditation, and another study examines a bottom-up approach centered on education-based, holistic rehabilitation programs tailored to individuals. Together, these approaches highlight two distinct channels for improving jail outcomes: reshaping institutional environments and empowering individual transformation.
Our joint work indicates that both pathways impact behavioral and health outcomes during and after incarceration and suggests innovative ways local law enforcement and communities can invest in jails to disrupt recidivism cycles and reduce mortality rates among incarcerated populations.
Voluntary Accreditation and Healthcare Quality in US Jails
As wards of the county or state during confinement, incarcerated individuals rely entirely on correctional institutions for medical care, and since the Supreme Court’s landmark decision in Estelle v. Gamble (1976), correctional institutions have been constitutionally obligated to provide it. Yet, most jails operate with limited medical oversight, and there is no dedicated funding for inmate healthcare due to the Medicaid Inmate Exclusion Policy. Healthcare delivery in jails is largely overseen by sheriffs with limited medical expertise and delivered through contracts with for-profit vendors under capitated payment structures. These conditions create incentives to reduce costs by cutting quality along dimensions that are noncontractible or difficult to monitor.
This combination of weak external monitoring and non-expert principals is particularly concerning in jail settings. Accreditation could provide standardized expertise and independent compliance assessments to help public officials monitor quality and constrain private service providers’ incentives to reduce noncontractible dimensions of quality. However, the effects of accreditation have only been studied in the US civilian health system and evidence remains mixed and non-causal.
In Alsan and Yang (2025), we conduct the first randomized controlled trial of healthcare accreditation and, to the best of our knowledge, the first randomized controlled trial in US jails, and evaluate its impact on process-based measures of quality and mortality.2 Over several years, we randomized the offer of accreditation to 46 midsized jails (average daily population between 100 and 3,000) across the United States. Facilities were randomly assigned to receive a subsidy to pursue accreditation from the National Commission on Correctional Health Care (NCCHC) either immediately or at the end of the study period. NCCHC standards of care are often regarded as a “gold standard” and, in some cases, as evidence of constitutionally adequate care, although critics argue that accreditation may be ineffective and even counterproductive.
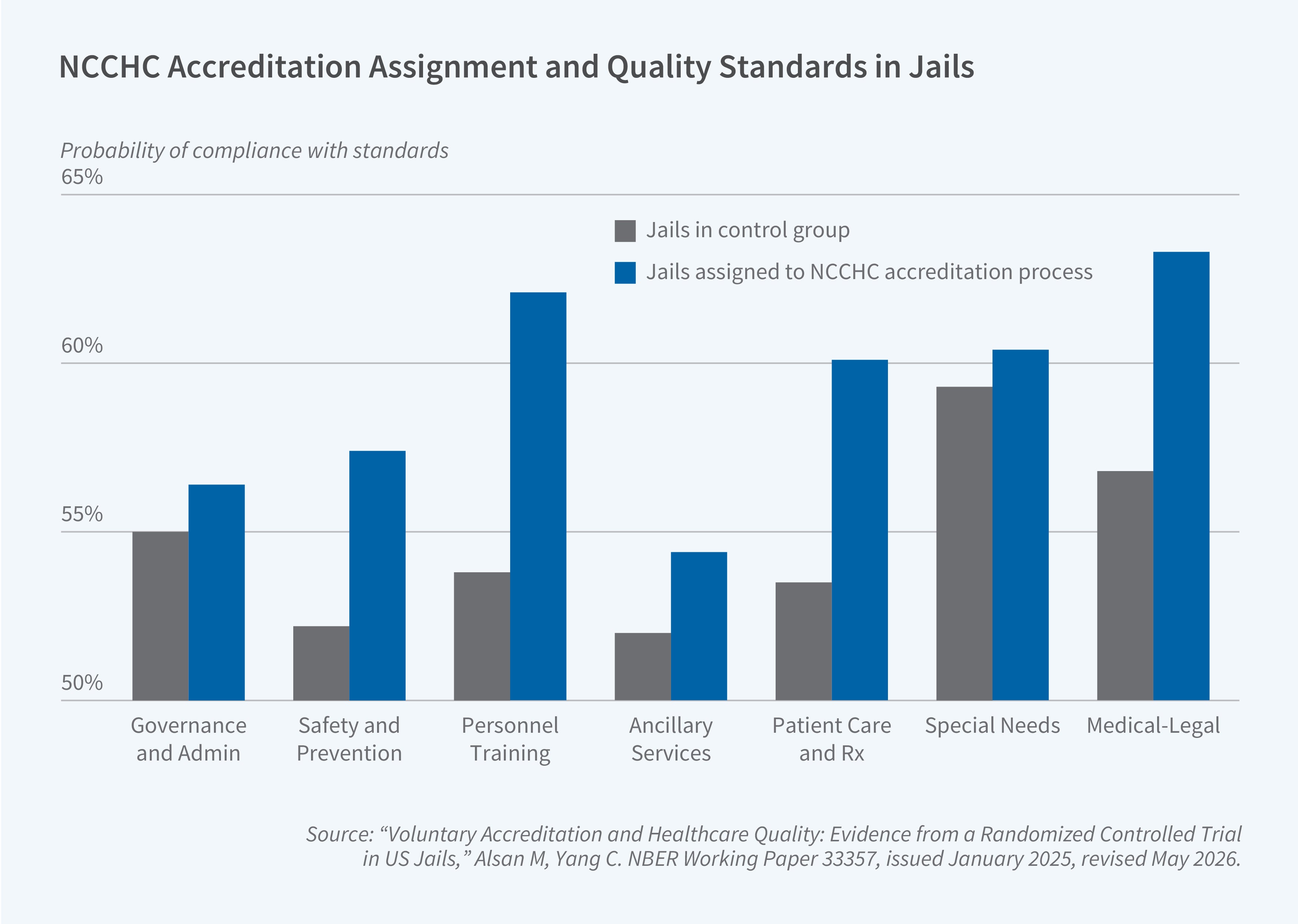
NCCHC standards span seven core categories ranging from governance and administration to patient care and treatment. We measured compliance and organizational practice using five primary instruments. We administered a detailed survey to jail leadership, conducted independent audits of medical records and death logs, and fielded anonymous surveys of medical and custody staff. At the end line, we conducted qualitative interviews with jail leadership and incarcerated individuals. We also conducted an incentivized survey of 145 experts across several domains—including jail administrators, healthcare providers, policy experts, and the formerly incarcerated—to elicit beliefs about the importance of different standards as well as predictions about the effects of compliance with standards. We prespecified three methods for constructing a meta-index using the individual indices of compliance with the NCCHC quality standards to address multiple hypothesis-testing concerns: a simple average across the seven NCCHC quality standard indices, a principal component analysis, and an expert-weighted average of the seven indices.
Effects on Quality Standards and Mortality
We find that assignment to the NCCHC accreditation process leads to statistically significant improvements in compliance with quality standards, particularly in training and patient care. We also find that treatment assignment yields statistically significant and medically meaningful increases across all three prespecified meta-indices.3 [See Figure 1]
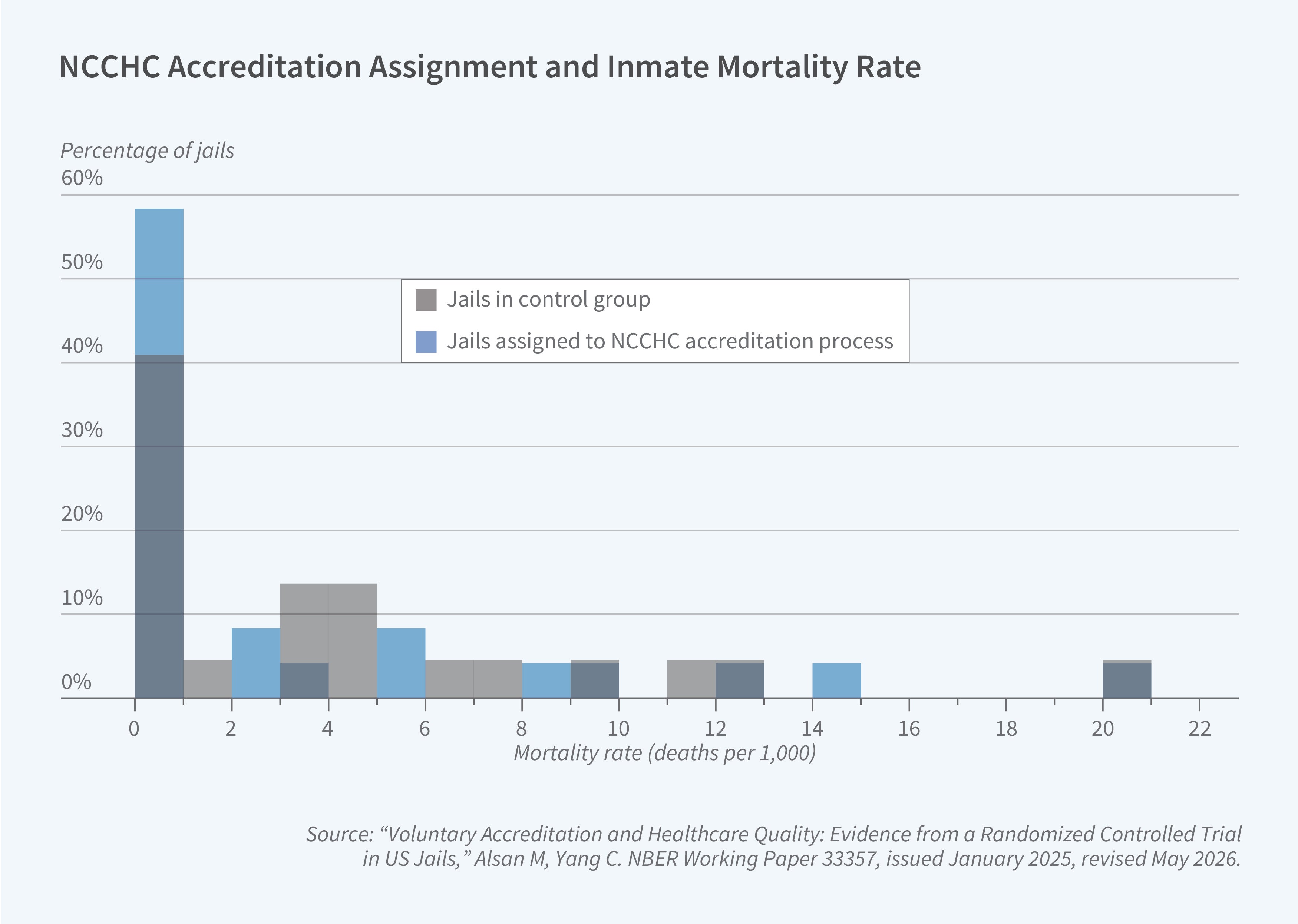
Assignment to the accreditation process also reduces the 12-month mortality rate (deaths per 1,000) in jails by approximately 60 percent, with the largest reductions concentrated in preventable causes and in jails that experienced the greatest quality improvements. Figure 2 presents the mortality rate distribution for treatment and control groups using administrative death logs and shows a leftward shift in the jails assigned to accreditation. This result is robust to different functional forms and holds across both the administrative death logs and our independently collected mortality data from media reports, mitigating concerns that our findings are driven by reporting bias.
Staff Coordination and Timely Screening
We find evidence that suggests effects operate through improving coordination between staff, timely screening, and increased information for oversight. Notably, these improvements are achieved without structural changes in inputs, such as increases in staffing or capital investments, reflecting the standards’ focus on organizational practices and procedures rather than new resources.
Staff surveys reveal that treatment assignment generates statistically significant improvements in horizontal coordination. In addition to more staff reporting coordination and communication between custody and medical staff, we also find positive improvements in staff feeling valued at work and sufficiently equipped with tools and resources. Interviews with facility leadership corroborate these patterns, with leadership highlighting the importance of knowing the correct protocols and securing buy-in from custody staff.
Consistent with our finding that treatment substantially reduces mortality associated with preventable causes, our independent medical audits find increased early screening for several acute and mental-health-related conditions, including withdrawal symptoms, chronic disease indicators, and suicide risk. Screening also substantially increased for three high-risk conditions: suicidal ideation, opioid use disorder, and hypertension. Correspondingly, accreditation assignment yields improvements in documentation and screening for mental health history and prior psychiatric or addiction treatment. In interviews with facility leadership at the jails, we found that the biggest changes reported by almost all treatment facilities were with respect to screening and initial health assessments, with some especially emphasizing mental health screening and processes of care.
While treatment assignment leads to changes in documentation and screening, it does not generate changes in staffing levels, healthcare vendors, or referral patterns for off-site care. However, treatment facilities do increase services for incarcerated individuals, (e.g., laboratory and pharmacy services), consistent with findings on improved screenings for medical conditions.
Overall, these findings reveal that the impact of accreditation operates through improved staff coordination, improved documentation and adherence to protocols, and increased early screening. The evidence also demonstrates that meaningful improvements in quality of care and mortality reductions are achievable without resource expansion or additional capital, and instead, through improvements in organizational practices.
Education-Focused Rehabilitation in Jail
The Inmate Growth Naturally and Intentionally Through Education (IGNITE) program represents a more bottom-up approach to reform, focusing on direct engagement with incarcerated individuals through education and cultural change. In September 2020, Sheriff Christopher Swanson of Genesee County, Michigan, launched the education-centered initiative. The initiative was designed to reverse the cycle of generational incarceration through education by restoring value, hope, and purpose to the incarcerated population. IGNITE is a voluntary, meritocracy-based approach to rehabilitation that relies on the community for support.
To estimate the effect of exposure to IGNITE, we and Barnett leveraged jail administrative data and a novel instrumental variable approach that exploits quasi-random variation in the length of jail stays caused by court scheduling delays.4 These court delays are caused by changes in the schedule of the judge or prosecutor assigned to the case, fiscal crises, or holidays and are uncorrelated with defendant characteristics or predicted recidivism risk. In our data, such delays extend jail stays by approximately two weeks on average, both before and after IGNITE’s launch. We used these delays as an instrument for program exposure and combined this approach with a difference-in-differences framework comparing outcomes before and after program implementation. This approach allowed us to isolate the causal effect of additional exposure to IGNITE.
Effects on Behavior and Recidivism
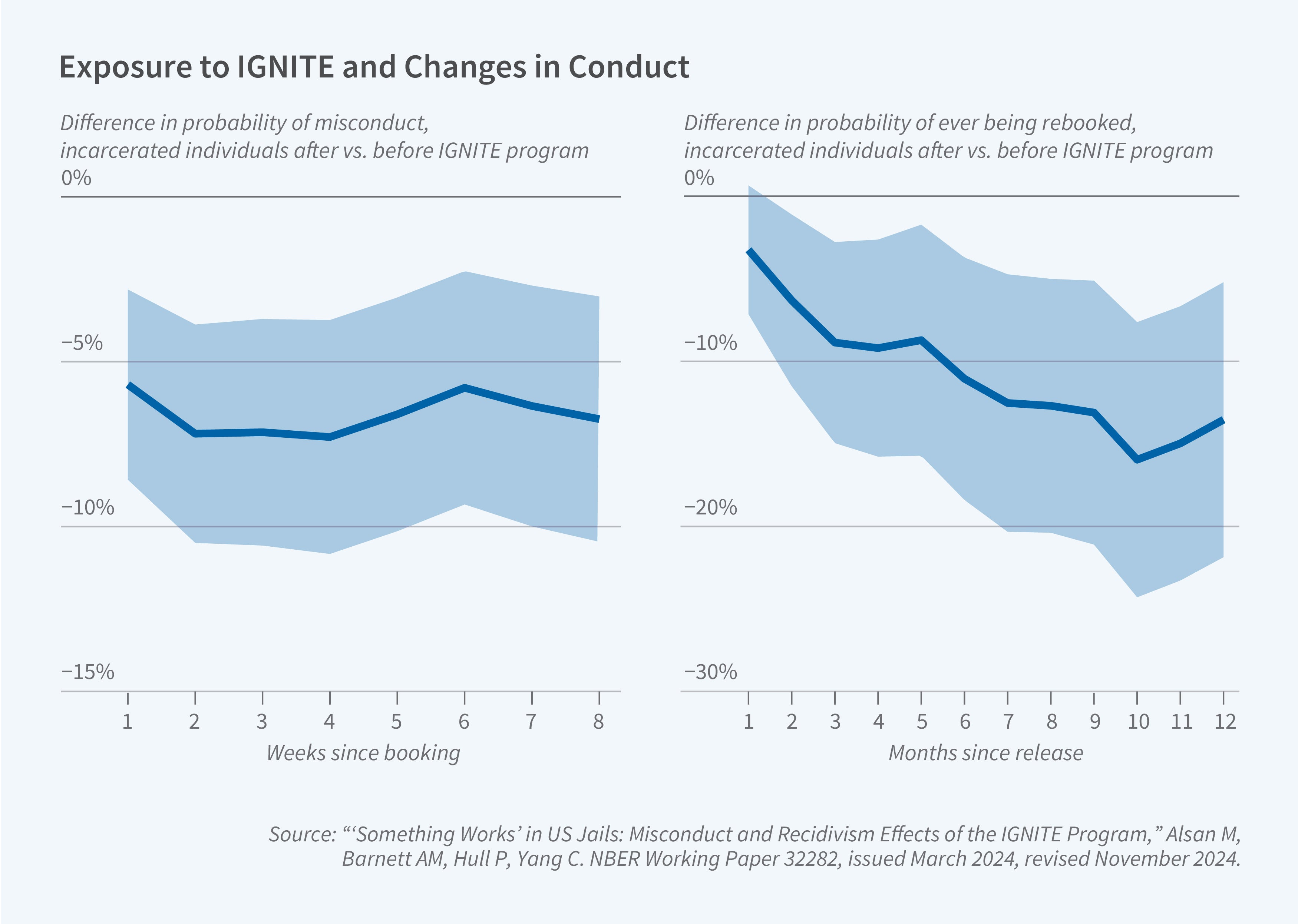
We find that exposure to IGNITE substantially reduces the likelihood of in-jail misconduct and recidivism.5 One additional month of exposure to the program reduces incidences of weekly major misconduct within the jail by 25 percent. The improvements in behavior extended beyond the facility walls. Each additional month of exposure reduces three-month recidivism by 24 percent (9 percentage points). We find similar misconduct and recidivism effects across different demographic groups, prior-offense status, and predicted exposure to the Flint water crisis. Reductions in rebooking persist for up to one year after release, the longest follow-up horizon available in the data. As shown in Figure 3, recidivism effects also grow over time, reaching a 14 percentage point reduction at one year, with the largest impacts among individuals with high predicted recidivism risk.6
Academic Achievement and Cultural Change
We further study the mechanisms underlying these results.7 First, we find that the individualized structure of IGNITE produces substantial gains in academic achievement. Participants advance roughly one grade-level equivalent in literacy and math assessment scores during their period of exposure. Second, evidence suggests that the program shifts attitudes and expectations for both incarcerated people and jail staff. Sentiment analysis of administrative text-message data exchanged between incarcerated individuals and jail staff shows that incarcerated individuals exposed to IGNITE are more likely to use language classified as positive and trust-related compared to those incarcerated before the program’s implementation. Our custody staff survey, which shows balanced exposure to IGNITE participants among respondents, reveals that officers with more frequent interaction with IGNITE participants are approximately twice as likely to view educational programming in jails as worthwhile as officers with limited interaction with IGNITE participants.
Consistent with the in-jail evidence, observed positive spillovers in the community suggest cultural change extending beyond the jail. Using our anonymized Flint community survey, which was conducted with no IGNITE association in our distribution channels or questionnaire, we assess respondents’ trust in local law enforcement. Community members who were formerly incarcerated or had a family member or close friend incarcerated in Genesee County Jail after September 2020 (indicating IGNITE exposure) are 23 percentage points more likely to express positive views of law enforcement than respondents without either experience.
These behavioral and attitudinal changes generate substantial social returns. We estimate that one additional month of IGNITE exposure reduces the three-month social cost of crime and incarceration by at least $2,954 per individual. Over a one-year horizon, the reduction in social costs amounts to at least $7,285 per person-month. Even under conservative assumptions, the implied social savings exceed $6,000 per participant, a strikingly large benefit relative to the modest cost of administering the program.
Following IGNITE’s demonstrated impact and positive rehabilitative benefits in Genesee County, Michigan, the National Sheriffs’ Association adopted the initiative and has replicated IGNITE in dozens of jails nationwide, customizing each site through local partnerships. Ongoing research examines IGNITE as it expands across the country.
Conclusion
Our collaborative research examines two distinct institutional investments in jails: a top-down strategy through external healthcare accreditation aimed at improving organizational practices and procedures, and a bottom-up strategy focused on education-based rehabilitation that promotes holistic individual growth and skill development among the incarcerated. Despite targeting different domains, both investments demonstrate that rehabilitative investments impact behavior and institutional culture in ways that can improve safety and behavioral outcomes. Both investments also highlight the interconnectedness between educational achievement and engagement and underlying health and wellbeing, as the capacity for incarcerated individuals to participate in programming is intertwined with whether their basic medical and mental health needs are being met.
Taken together, these findings demonstrate that institutional reforms within local jails can yield outsize benefits across multiple dimensions: improved facility safety, reduced recidivism, reduced mortality, and improved community perception of law enforcement. These benefits, both during and after the period of incarceration, demonstrate the value of rehabilitative approaches within the criminal justice system.
Endnotes
“What Works? — Questions and Answers About Prison Reform,” Martinson R. The Public Interest 35, Spring 1974, pp. 22-54.
“Voluntary Accreditation and Healthcare Quality: Evidence from a Randomized Controlled Trial in US Jails,” Alsan M, Yang C. NBER Working Paper 33357, issued January 2025, revised May 2026.
“‘Something Works’ in US Jails: Misconduct and Recidivism Effects of the IGNITE Program,” Alsan M, Barnett AM, Hull P, Yang C. NBER Working Paper 32282, issued March 2024, revised November 2024, and The Quarterly Journal of Economics, 140(2), May 2025, pp. 1367-1415.


