The Health and Healthcare Spending Effects of GLP-1s
Glucagon-like peptide-1 receptor agonists (GLP-1s), better known by brand names such as Ozempic and Wegovy, have generated intense interest as potentially transformative treatments for type 2 diabetes and obesity. Clinical trials found substantial weight loss and improved cardiovascular outcomes associated with taking these medications. Two new studies estimate how these drugs affect health outcomes and medical care costs in the broad population.
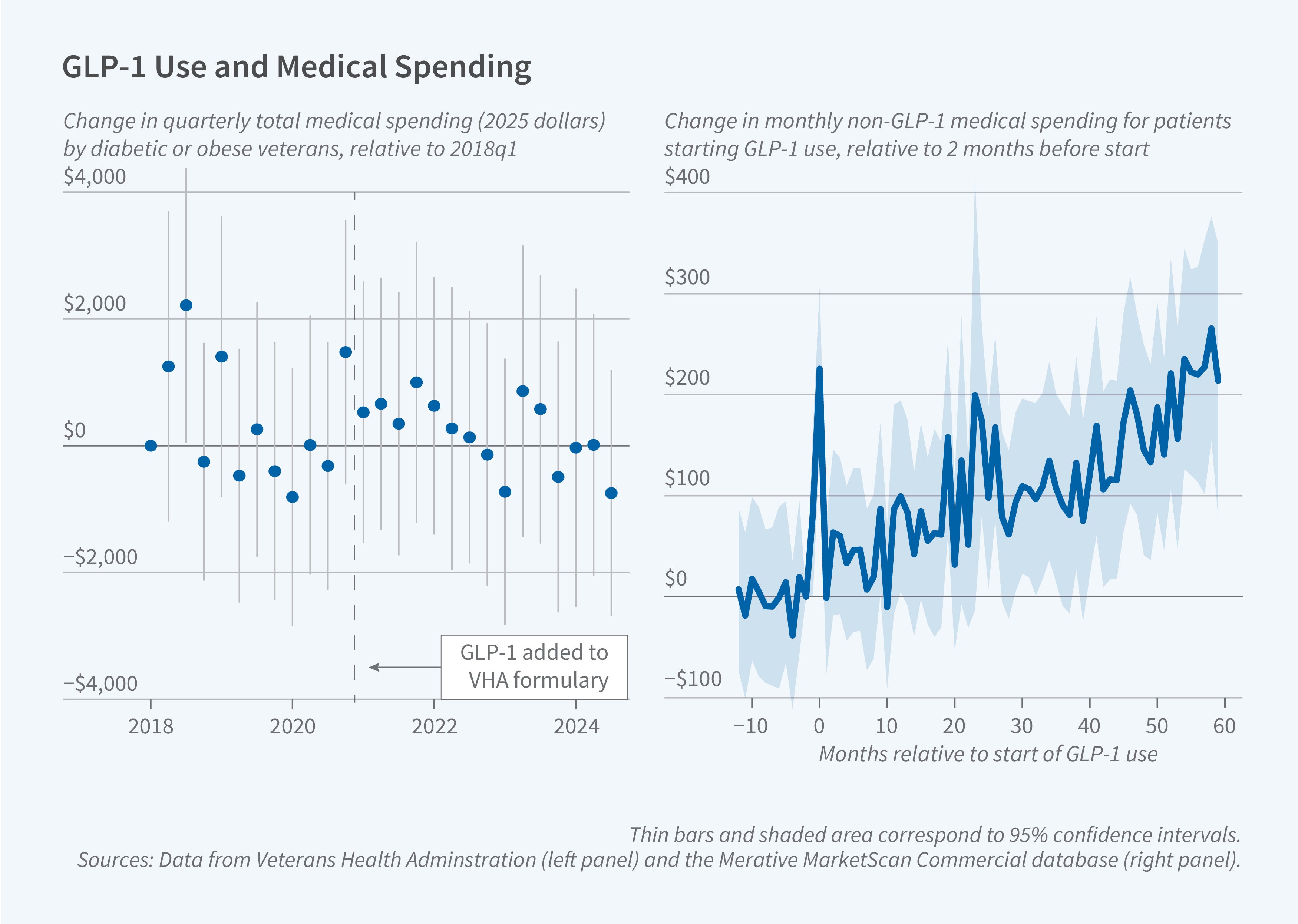
In Weighing the Impacts of GLP-1s: Quasi-Experimental Evidence from Provider Adoption (NBER Working Paper 34667), Sam Bock, Jasmin Moshfegh, and Jonathan Zhang study 1.4 million veterans who were diagnosed with diabetes or obesity and who received care through the Veterans Health Administration (VHA). The researchers exploit variation in prescribing patterns among VHA primary care providers following the addition of GLP-1s to the VHA formulary in November 2020. They measure each patient's existing 2018 primary-care provider's propensity to adopt GLP-1s by calculating that provider’s likelihood of prescribing GLP-1s in the 2021–22 period. Then, they compare outcomes between patients with 2018 providers who were high- and low-adopting practitioners. Patients whose providers became "always-adopters," prescribing GLP-1s frequently, were 20 percentage points more likely to fill GLP-1 prescriptions in 2023–24 than those with providers who never prescribed GLP-1s.
The estimated effects on blood glucose and body weight were largest in 2021, immediately after GLP-1s were included in the VHA formulary. A 30-week dose of GLP-1 results in a 3.3 percent loss of weight and a drop in blood glucose A1C of 0.32 percentage points, changes that closely match clinical trial results. Over time, however, the treatment effect of a marginal 30-week regimen dissipated. By 2024, the associated weight loss was only half as large as the 2021 estimate, and the effect on A1C was not statistically different from zero. This attenuation is explained in part by shifting complier composition: As GLP-1 diffusion expands, the marginal patients induced into treatment become progressively healthier.
Despite the metabolic improvements, the study finds no evidence of broader health improvements or utilization changes in data up to and including 2024. Although the researchers replicate a clinical trial finding of a reduction in heart attacks and strokes among patients with existing cardiovascular disease and chronic kidney disease and a reduction in moderate alcohol consumption risk, they find no statistically significant decline in broader emergency department visits or in any major diagnostic category. Mental health measured via clinical questionnaires is also unchanged. Notably, the researchers do not observe changes in total non-medication, non-GLP-1 medical spending.
In a second study, Do GLP-1 Medications Pay for Themselves? (NBER Working Paper 34678), Coady Wing, Sih-Ting Cai, Daniel W. Sacks, and Kosali I. Simon analyze commercial insurance claims for approximately 537,000 patients who initiated GLP-1 treatment between 2017 and 2022. They compare patients initiating treatment in a given month to those who initiate 12 months later in a one-year follow-up design and 60 months later in a five-year follow-up design, allowing them to control for underlying time trends and baseline health differences. They find that patients spend approximately $1,000 on GLP-1s in their initiation month, but many discontinue treatment within the first few months. The share with active supply stabilizes at about 60 percent after three months and 56 percent after one year. Accounting for discontinuation, cumulative GLP-1 spending is about $6,500 in the first year and $22,500 over five years.
The researchers find no reduction in overall healthcare spending following GLP-1 initiation. In fact, in the first year after initiation, total non-GLP-1 spending increases by $585. The spending increase is driven primarily by higher outpatient costs, an increase of $438 in the first year, likely reflecting monitoring visits for dose titration and managing side effects. While GLP-1 initiation reduces spending on other diabetes medications by $189 annually, this offset is insufficient to counterbalance increased outpatient costs. Over five years, non-GLP-1 spending increases by $6,800, or 30 percent of the amount spent on GLP-1s. The pattern persists across patient subgroups, including those with diabetes, cardiovascular disease, and obesity diagnoses.
The researchers conjecture that the difference between the findings for broader health improvements in GLP-1 clinical trials and in the rollout of these drugs in the general population may result from greater adherence to the GLP-1 regimen for those in clinical trials and from differences in the treatment populations. Relative to participants in clinical trials, patients receiving GLP-1s in the general population are probably healthier, with less scope for short-run health improvements and cost savings.
The authors of “Weighing the Impacts of GLP-1s: Quasi-Experimental Evidence from Provider Adoption” acknowledge support from the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowships, and Jasmin Moshfegh acknowledges support from The Big Data Scientist Training Enhancement Program.
The authors of “Do GLP-1 Medications Pay for Themselves?” acknowledge support from Indiana University’s Health Excellence Achieved through Learning Health Systems Research (HEALeR) Collaborative, and the National Institute for Healthcare Management Foundation.