The Impact of Paid Family Leave on Families with Health Shocks
The US is one of the few countries worldwide that does not have a federal paid family leave (PFL) policy. In the absence of a federal policy, some states have adopted PFL policies, starting with California in 2004 and now including 11 states and the District of Columbia. These PFL policies provide paid time off for workers who need to care for a newborn or a newly adopted child (parental leave) or for an ill or temporarily disabled family member (caregiving leave).
While there is extensive research on the use of PFL for parental leaves, based on the experience of California and other early adopting states, much less is known about the use of PFL for caregiving leaves. The imbalance in empirical evidence for the two types of leaves may contribute to the higher level of public support and greater consensus among policy experts as to the value of parental leaves as compared to caregiving leaves.
In The Impact of Paid Family Leave on Families with Health Shocks (NBER Working Paper 30739), researchers researchers Courtney Coile, Maya Rossin-Slater, and Amanda Su aim to add to the limited evidence base on caregiving leaves.
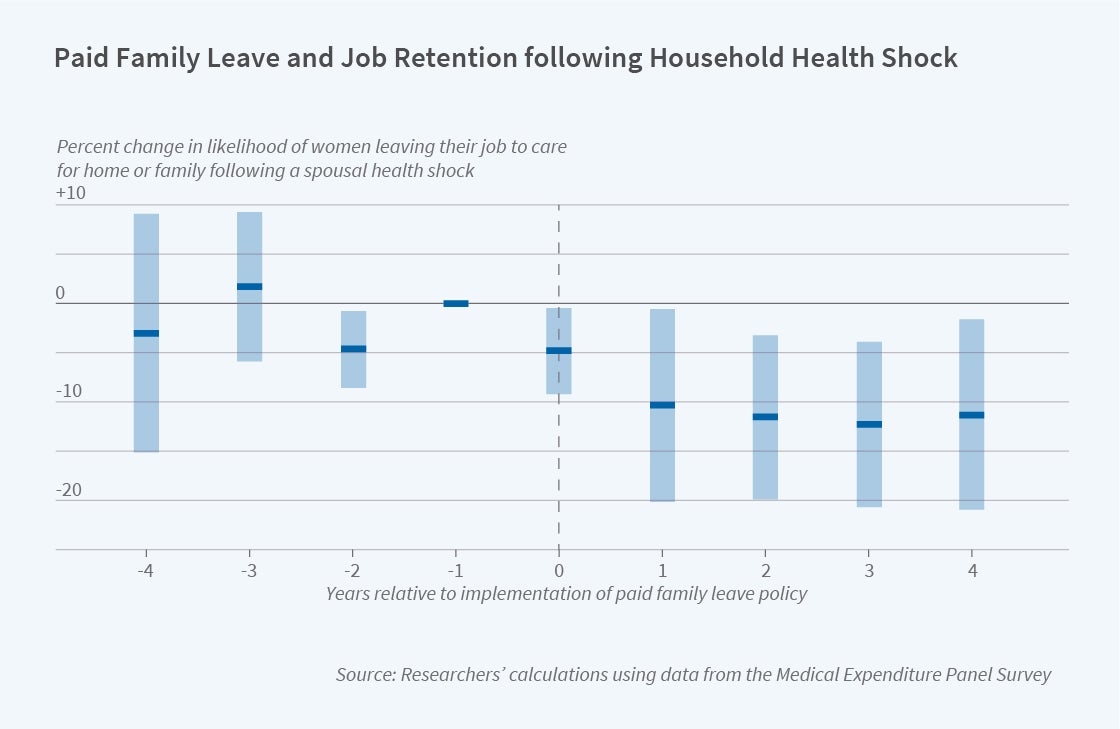
The authors focus on the effect of PFL access in California, New Jersey, and New York, three of the earliest adopting states. They use 1996–2019 data from the Medical Expenditure Panel Survey to identify workers whose spouse or child experiences a health shock — defined as a hospitalization or surgery — during the two years that households are followed in the survey. In their empirical analysis, they compare the differences in post-health-shock labor market and mental health outcomes of these workers before and after the implementation of PFL in their state, relative to analogous differences among workers in states with no change in PFL access.
The authors find that having access to PFL leads to a 7.0 percentage point decline in the probability that working wives whose spouse has a hospitalization or surgery report “leaving a job to care for home or family” in the survey interviews following the health shock. For men, there is no such effect. This gender difference in the effect of PFL access is consistent with previous literature that has found that women are substantially more likely to engage in caregiving for their ill spouses than men. Interestingly, the effects of PFL access on employment are concentrated among spousal caregivers with low levels of education, suggesting that government-provided PFL may reduce pre-existing disparities in leave use and associated outcomes.
Evidence on mental health impacts of PFL access is more mixed. Some specifications suggest that PFL access leads to a large reduction in the likelihood of reporting poor mental health or of using a mental-health-related prescription following a health shock for women and caregivers with less education — the same groups for which PFL access affects job continuity. However, these findings do not hold up across all specifications.
In contrast to results for spousal caregivers, there is no evidence that PFL access affects labor market or mental health outcomes of parental caregivers. Future research should continue to study the needs of working parents whose children experience health shocks and how PFL policies may better serve these families. Research is also needed to understand the use of PFL to manage parental health challenges, a critical issue given the large share of working women who contend with parental caregiving responsibilities at some point.
Overall, this study suggests “that when spouses with a medical condition or limitation experience a hospitalization or surgery, having PFL access enables (healthy) wives to care for them while retaining their jobs.”
The research reported herein was performed pursuant to grant RDR18000003 from the US Social Security Administration (SSA) funded as part of the Retirement and Disability Research Consortium. The opinions and conclusions expressed are solely those of the author(s) and do not represent the opinions or policy of SSA, any agency of the federal government, or NBER. Neither the United States Government nor any agency thereof, nor any of their employees, makes any warranty, express or implied, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of the contents of this report. Reference herein to any specific commercial product, process or service by trade name, trademark, manufacturer, or otherwise does not necessarily constitute or imply endorsement, recommendation or favoring by the United States Government or any agency thereof. This project was also supported by grant number T32HS026128 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. The views expressed herein are those of the authors and do not necessarily reflect the views of the National Bureau of Economic Research.


