Health Effects of Managed Care Delivery for Medicaid’s Long-Term Services and Supports
With the aging of the US population, demand for medical and nonmedical assistance with basic daily activities is high and rising. Medicaid bears over 60 percent of the costs of this assistance, paying $255 billion in 2022 for long-term services and supports (LTSS). In response to these costs, some state Medicaid programs have shifted delivery of these services from fee-for-service to managed care.
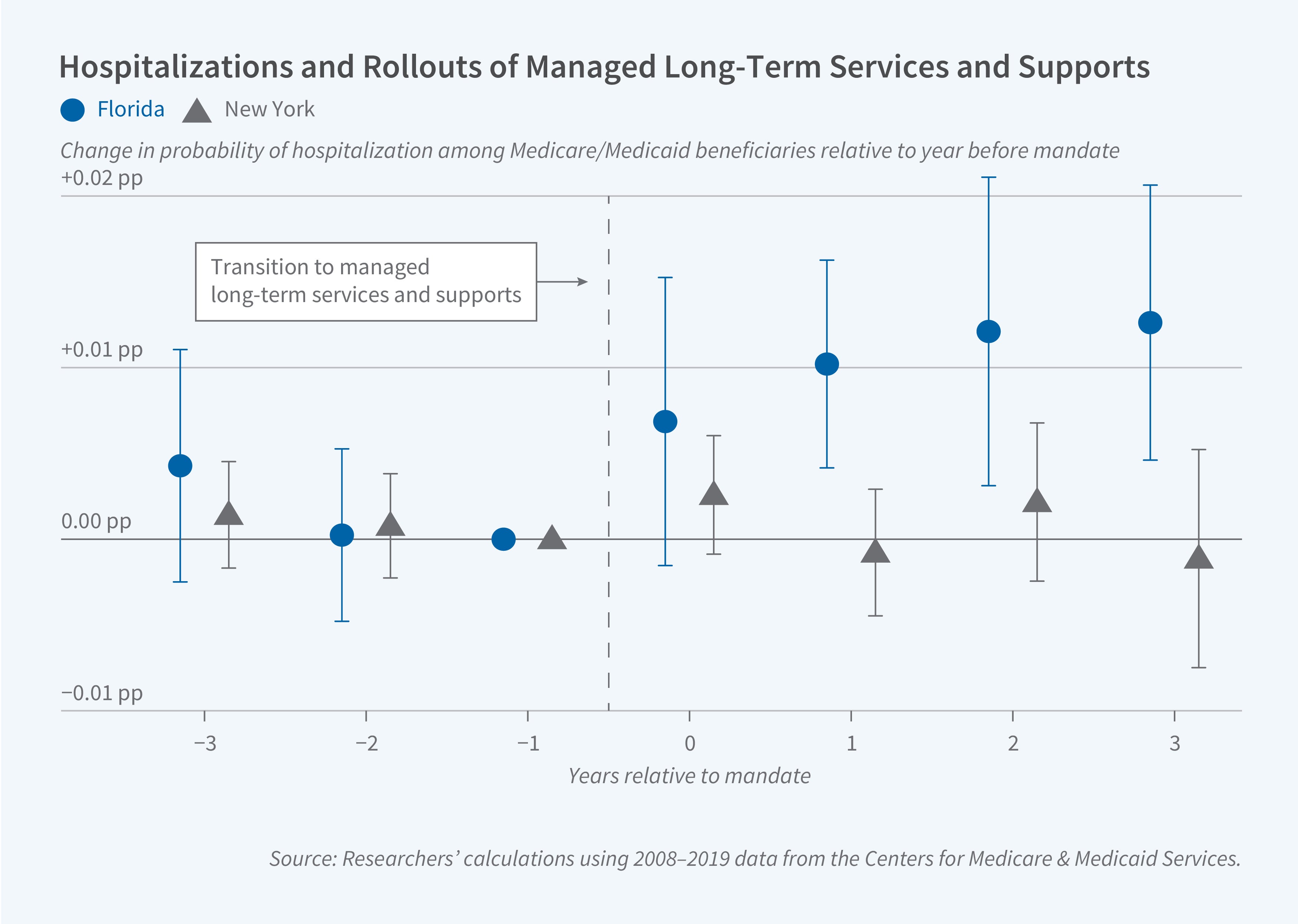
The shift to a managed care model for delivery of long-term services and supports was associated with a 0.9 percentage point (4.2 percent) increase in the quarterly risk of a hospitalization in Florida, but there was no discernible impact in New York.
Under managed care, private plans receive fixed monthly payments from Medicaid to assume responsibility for providing LTSS for each qualified recipient. In addition to forming provider networks and implementing gatekeeping strategies, these plans typically provide case managers to coordinate care, whether in nursing homes or in home- or community-based settings.
Both Florida and New York implemented a staggered county-by-county rollout of managed LTSS between 2012 and 2015. Using administrative Medicare data, Ajin Lee, Maya Rossin-Slater, Becky Staiger, and Amanda Su assess the health effects of these transitions in The Impacts of Medicaid’s Managed Long-Term Services and Supports on Health Outcomes in Medicare (NBER Working Paper 35055). They compare changes in hospitalization rates for elderly enrollees who were dually eligible for Medicare and Medicaid in counties that adopted managed LTSS to changes in hospitalization rates for comparable enrollees in Pennsylvania and California counties that did not.
The shift to managed LTSS was associated with a 0.9 percentage point (4.2 percent) increase in the quarterly risk of a hospitalization in Florida, but there was no discernible impact in New York. The increased hospitalizations were concentrated among respiratory diagnoses and other urgent conditions, with admissions typically originating in the emergency department.
Since hospitalizations are primarily financed by Medicare and are not directly affected by the incentives of managed LTSS, the researchers interpret the increase in hospitalization rates in Florida as an indication of deteriorating health status. The rise in hospitalization rates also demonstrates that the transition to managed LTSS can have effects that extend beyond the Medicaid program, spilling over to Medicare-financed services.
The researchers examine several possible channels for the increase in hospitalizations, including changes in patterns of nursing home or preventive care utilization. They do not find any evidence of changes in nursing home use, switching, or quality. However, they report that managed LTSS was associated with a 3.2 percentage point (10 percent) decline in the likelihood that Florida enrollees were vaccinated against influenza. There was no comparable change in flu vaccinations in New York. The researchers suggest that the differential decline in flu vaccinations in Florida, perhaps reflecting differences in case management practices, could explain the increase in urgent hospitalizations for respiratory diagnoses there.
Given the heterogeneous nature of their findings, the researchers conclude that “managed LTSS is not a uniform model, and its impacts depend on how states design and implement their programs.”
The researchers acknowledge financial support from the National Institute on Aging of the National Institutes of Health under award number R01AG077949. Su acknowledges support from the National Science Foundation Graduate Research Fellowship Program under grant number DGE-1656518.


