Institutional Special Needs Plans for Nursing Home Residents with Dementia
At any given time, nearly 1 million Americans reside in a nursing home and receive long-term care, with most having some form of dementia. Nursing homes operate under fragmented financing where Medicare pays for post-acute care only after a three-day hospitalization, while Medicaid or private payments cover long-term care. This system discourages investment in on-site clinical capabilities and encourages facilities to transfer residents to hospitals for treatment of acute illnesses. In 2022, post-acute care margins for nursing homes were 22 percent compared to an overall margin of –1.3 percent across all payers, creating strong financial incentives to hospitalize residents to access higher Medicare payments. Consistent with these incentives, these facilities face persistently high hospitalization rates.
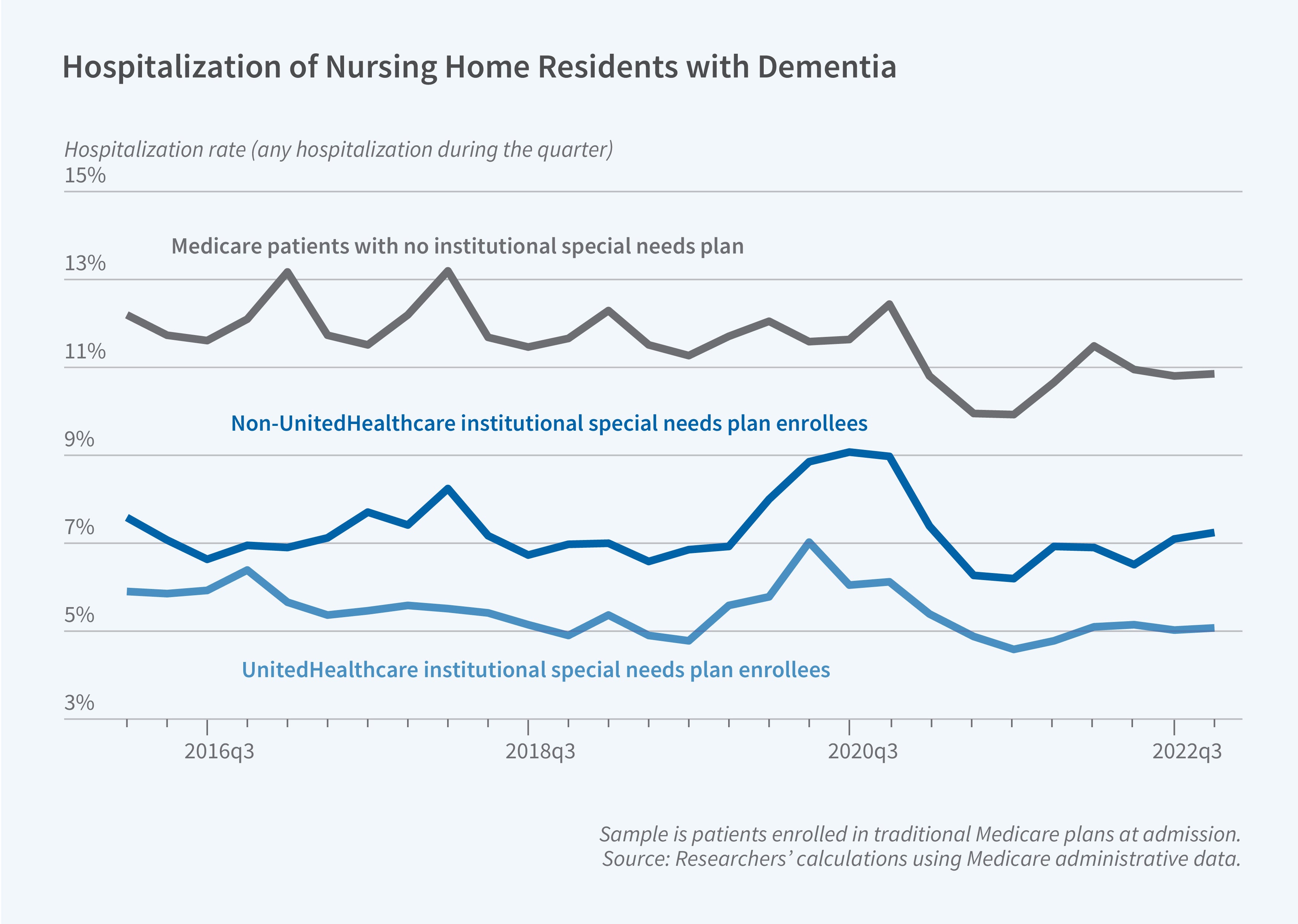
In Is Managed Care Effective in Long-Term Care Settings? Evidence from Medicare Institutional Special Needs Plans (NBER Working Paper 34235), Momotazur Rahman, Brian McGarry, Elizabeth M. White, David C. Grabowski, and Cyrus M. Kosar examine whether Institutional Special Needs Plans (I-SNPs) can reduce hospitalizations while maintaining care quality. I-SNPs are Medicare Advantage plans designed exclusively for individuals certified as requiring facility-based long-term care. Unlike traditional Medicare, I-SNPs receive capitated payments and eliminate the three-day hospitalization requirement for post-acute care coverage, creating incentives to reduce costly hospital use. Additionally, I-SNPs must operate a Medicare-approved clinical model of care which includes employing advanced practice clinicians who work on-site in nursing homes to coordinate care and treat acute illnesses in place. The share of long-stay nursing home residents enrolled in I-SNPs quadrupled between 2006 and 2021, from 2.2 percent to 8.8 percent. The largest and oldest I-SNP is operated by UnitedHealthcare (UHC), but more recent growth has been driven by non-UHC plans.
Enrollment in Institutional Special Needs Plans reduces quarterly hospitalization rates by about 3 to 4 percentage points among long-stay nursing home residents with dementia.
The researchers analyzed 12 million resident-quarter observations from 2016 through 2022. They examined long-stay nursing home residents aged 65 and older with Alzheimer's disease and related dementias and compared outcomes for residents before and after their facility began offering I-SNPs. When I-SNPs were offered, individual enrollment increased by approximately 20 percentage points. For residents who entered a nursing home with conventional Medicare Advantage coverage, I-SNP enrollment decreased hospitalization by approximately 3 percentage points. Among residents who entered nursing homes enrolled in traditional Medicare, I-SNP enrollment reduced quarterly hospitalization rates by roughly 4.3 percentage points.
For UnitedHealthcare I-SNPs, the probability of hospitalization fell by between 3.5 and 4.1 percentage points for Medicare Advantage entrants and by around 4.5 percentage points for traditional Medicare entrants. Non-UHC I-SNP enrollment yielded smaller effects of around 2 percentage points for Medicare Advantage entrants and between 3.0 and 3.6 percentage points for traditional Medicare entrants. Using a hospitalization measure based on nursing home discharge assessments, the researchers find that I-SNP enrollment reduced the probability of discharge to any inpatient facility by roughly 2.9 percentage points and 4.3 percentage points for residents originally enrolled in conventional Medicare Advantage plans and traditional Medicare, respectively. The magnitude of the hospitalization reductions increased the longer an I-SNP was present within a nursing home, indicating growing effectiveness as partnerships between plans and nursing homes developed.
The researchers did not find any evidence that I-SNP enrollment raised the risk of adverse secondary outcomes. Using baseline hospitalization rates and average Medicare hospitalization costs, the researchers estimate that approximately 80,000 hospitalizations out of 240,000 could have been avoided with I-SNP enrollment, translating to $1.2 billion in savings for Medicare.
The researchers acknowledge support from the National Institutes of Health’s National Institute on Aging grants R01AG082098 and R01AG089051.


