Allocating Donor Kidneys to Maximize Years of Life Saved
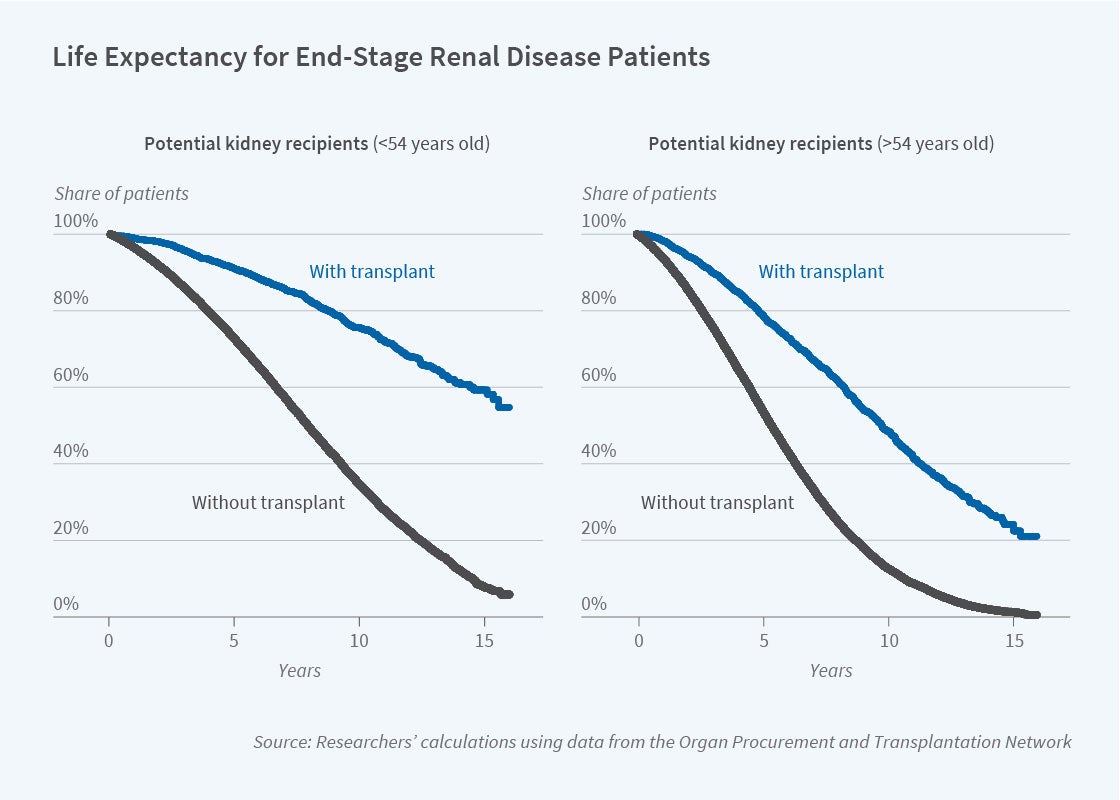
The current deceased donor kidney allocation system prolongs recipients’ lives by an average of 8.8 years. Alternative allocation rules could raise this substantially.
The process by which kidneys from deceased donors are allocated among potential recipients is an example of a resource allocation problem that does not rely on prices but that has attracted substantial interest from economists. About 100,000 patients in the United States currently are suffering from kidney failure and awaiting life-saving transplants. In a typical year, only about one-fifth of those in need receive such transplants.
In Choices and Outcomes in Assignment Mechanisms: The Allocation of Deceased Donor Kidneys (NBER Working Paper 28064), Nikhil Agarwal, Charles Hodgson, and Paulo Somaini investigate the survival outcomes associated with the mechanism for allocating deceased donor kidneys and compare it with two alternative allocation rules. One alternative is a random assignment process, essentially a lottery in which all patients on the waiting list have an equal chance of receiving an available kidney. It provides a lower bound for the number of years that could be added to patients’ lives through transplantation. The other alternative is an algorithm that maximizes the number of additional years of life from kidney transplants.
The researchers compare the outcomes of these three allocation procedures by studying the choices patients and their doctors make when offered an available kidney. Because patients and available kidneys differ on a number of dimensions, the match between the potential recipient and the available kidney matters. Many potential recipients, in consultation with their doctors, turn down available kidneys, opting instead to remain on the waiting list in the hope that a better match will be forthcoming. The researchers also model the number of years potential recipients are likely to survive without a transplant, and the post-transplant years of survival that are likely to result from accepting a given available kidney.
The researchers estimate that if kidneys were allocated randomly to potential recipients, the average recipient would experience 7.9 years of life extension. They also estimate that the assignment mechanism results in an average life expectancy gain of 8.8 years. This is because, relative to random allocation, the process matches patients who will benefit more from the transplant of a particular kidney to such a well-suited donation. Most of this gain in life extension, relative to random allocation, comes from allowing patient choice. Assignment to patients based on existing priority rules without allowing for patient choice would only generate an average of 8.0 years of life extension.
The researchers also ask what would happen if kidneys were allocated to potential recipients based only on the criterion of maximizing the number of additional years of life expectancy. Their calculations suggest that it would be possible to achieve an average life extension per kidney recipient of up to 13.8 years, but that doing so would involve significant changes from current procedures. Maximizing the life expectancy gains requires assigning transplants to patients who are relatively healthy and who would live longer without a transplant than many other potential recipients on the kidney wait-list. This highlights a key tradeoff in the kidney allocation process: maximizing survival benefits requires restricting the availability of transplants for sicker patients because those patients are expected to live fewer years after receiving a transplant.
The researchers point out that increasing the expected longevity of the roughly 13,000 annual deceased donor kidney recipients in the US can create substantial value. If a statistical life year is valued at $300,000, the gains from the current system relative to random assignment are worth approximately $3.5 billion per year. This calculation does not include the cost saving from reduced dialysis. Modifying the assignment process in a way that generates another year of life extension, on average, would be worth nearly $4 billion per year.
— Lauri Scherer


