Blue Laws, Religious Observance, and Health Outcomes
A sharp increase in “deaths of despair” — deaths from poisonings, suicides, and alcoholic liver disease — occurred in the US in the early 2000s, but the initial rise began a decade earlier for middle-aged Whites. These developments are studied in Opiates of the Masses? Deaths of Despair and the Decline of American Religion (NBER Working Paper 30840). In this paper, Tyler Giles, Daniel M. Hungerman, and Tamar Oostrom examine the relationship between the increase in such deaths and the widespread decline in religious practice that began in the late 1980s, also predominantly among middle-aged Whites.
To address the possibility of a third factor causing both the drop in churchgoing and the rise in mortality rates, the researchers study the effect of repealing “blue laws” that regulated commerce at certain times of the week, often Sunday mornings. After the Supreme Court determined that such laws could be unconstitutional, many were repealed. Using religiosity data from the General Social Survey (GSS) and information on blue law repeals in 24 states from 1973 through 2000, the researchers find that these repeals reduced religiosity, particularly among those aged 45 to 64. Blue law repeals were followed by an average 9 percentage point decline in weekly church attendance by this group, a 7 percentage point increase in infrequent attendance, an 11 percentage point decline in strong religious affiliation, and a 19 percentage point increase in weak or no religious affiliation. The decline in religious practice was greatest for the group that experienced subsequent increases in mortality: middle-aged Whites without college degrees.
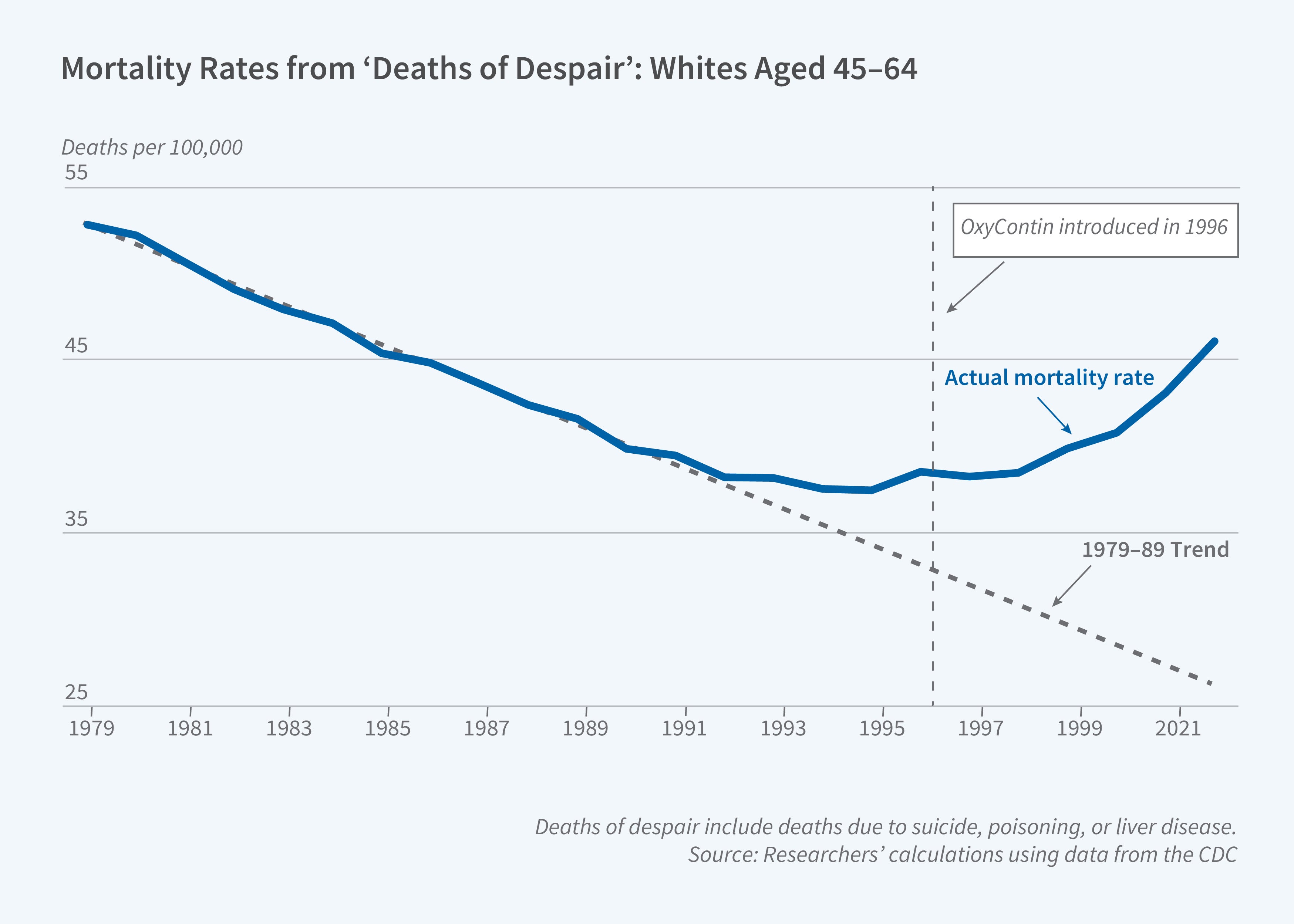
Falling church attendance is associated with a rise in mortality from "deaths of despair" among middle-aged Whites in the mid-1990s.
Using data from the Centers for Disease Control and Prevention’s Multiple Cause of Death files, the researchers track deaths, focusing on those caused by nondrug suicides, liver cirrhosis, and drug poisonings from 1969 through 2000. They find a steady linear decline in the 1980s for Whites aged 45 to 64, followed by a sharp reversal in the 1990s, both absolutely and relative to trend. The death rate was about 5 per 100,000 above trend by the mid-1990s. Using difference-in-difference models, the researchers find that changes in religious practice after blue law repeals were correlated with changes in mortality rates. For those aged 45 to 64, they find an increase of about 2 per 100,000 in deaths of despair associated with blue law repeals. The observed decline in weekly church attendance could therefore explain 40 percent of the rise in mortality from deaths of despair for this group in the mid-1990s.
Most of the blue law repeals were in the 1980s, prior to introduction of the opioid OxyContin in 1996, which dramatically increased overdose deaths. This may explain why the findings were strongest for suicide, in contrast to accidental drug-related deaths. The drops in religiosity and increases in deaths of despair did not differ by gender, and may have been slightly greater in rural areas.
To study whether changing death rates were associated with changes in spiritual beliefs rather than social religious participation, the researchers examine trends in self-reported personal prayer in the GSS. The fraction of individuals reporting praying at least every day remained relatively stable over this time period, suggesting that the decline in religiosity primarily stemmed from decreased participation in organized religion rather than changes in personal spiritual habits.
The findings point to the importance of cultural institutions in promoting well-being and mitigating mortality risks. The decline in religiosity during the 1990s may have diminished the capacity of religious communities to provide mutual insurance and other external benefits. This effect may have been larger for those in middle age, who on average have smaller social networks than younger adults.
— Susan Stewart
This study was funded by the National Institute on Aging under Grant Number T32-AG000186, the National Science Foundation Graduate Fellowship Program under Grant Number 1122374, and the Church Sexual Abuse Crisis Research Grant Competition.