Parental Dementia and the Wellbeing of Adult Children
Alzheimer's disease and related dementias (ADRD) currently affect nearly 50 million people worldwide. This number is expected to grow substantially in coming decades. While direct medical expenses of ADRD are well documented, the full societal burden includes a variety of impacts on family members. Standard cost estimates typically capture only foregone wages from hands-on caregiving, overlooking broader effects on relatives' wellbeing, including mental health consequences, that may persist for years.
In Family Spillovers of Dementia (NBER Working Paper 34635), Onur Altındağ, Jane Greve, and Yulya Truskinovsky examine how parental dementia affects adult children's labor market outcomes, physical health, and mental health. Using population-wide administrative data from Denmark spanning the period from 1995 to 2018, they identify all individuals who died with an ADRD diagnosis between 2005 and 2011 and link them to their adult children, resulting in a sample of 36,112 children whose parent died with dementia. Each adult child is matched to a demographically similar individual whose parent neither had ADRD nor died in the same year. The researchers track outcomes in the 10 years before and seven years after the parent's death.
In Denmark, having a parent with dementia does not affect adult children's labor market activity or physical health, but increases mental healthcare use—particularly among daughters.
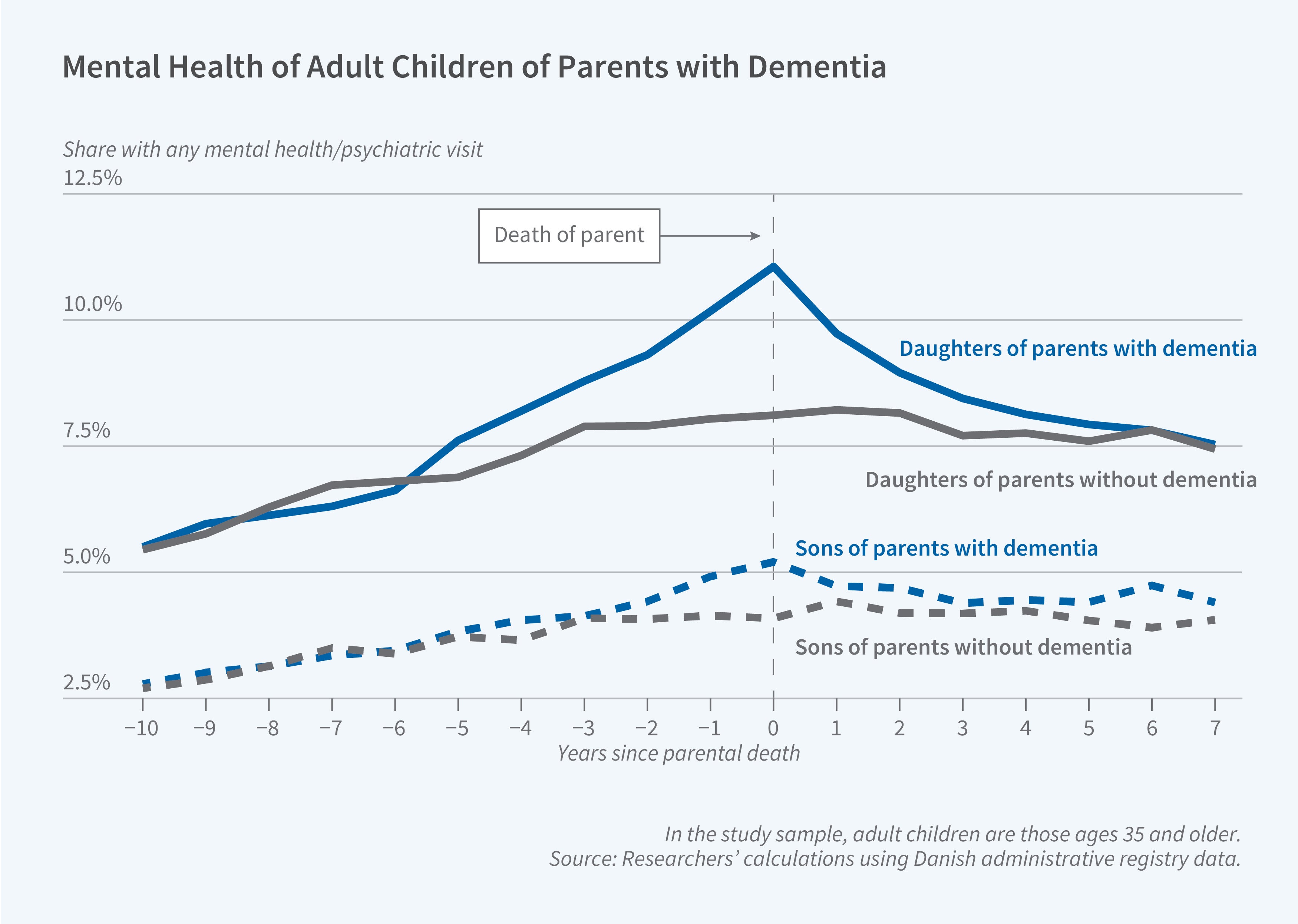
The researchers do not find any meaningful differences in labor supply, earnings, or physical healthcare use between the children of parents with ADRD and the control group. In contrast, mental healthcare use is substantially greater, particularly among women who have parents with dementia. Mental health–related visits among these women begin diverging from the control group approximately five years before a parent's death. Four to five years before a parent dies from ADRD, their daughters are 0.77 percentage points more likely to have a mental health visit, representing a 10 percent increase relative to the baseline rate of 7.7 percent. This rises to 1.12 percentage points (14.6 percent) two to three years before death and peaks at 2.17 percentage points (28.3 percent) during the three-year window surrounding the parent's death. Psychiatric medication use follows a similar pattern, increasing by 0.65 percentage points (3.8 percent) four to five years before death and reaching 1.27 percentage points (7.4 percent) around the time of death. This reflects greater use of antidepressants, anxiolytics, and hypnotics rather than antipsychotics. Effects are concentrated among women who lose a parent before age 50 and those with a college education, though effects appear across all education levels.
For men, whose baseline mental healthcare use is substantially lower, effects are more muted and concentrated around the year of parental death. Mental health visits increase by 0.66 percentage points (16.7 percent) and psychiatric prescriptions by 0.67 percentage points (6.6 percent) during the three-year period surrounding death, with some evidence of persistence for up to seven years after the parent’s death.
The researchers compare their findings with those from a larger sample of 195,687 individuals whose parents died without ADRD. Parental death from non-ADRD causes produces sharp but short-lived increases in mental healthcare use concentrated around the year of death, contrasting with the decade-long elevation observed for ADRD-related deaths.
The researchers acknowledge seed funding from the Hopkins Economics of Alzheimer’s Disease & Services Center and the Bentley University Research Council, and full funding from the Independent Research Fund Denmark.


