Fragmentation in the Delivery of Health Care
Having multiple providers involved in a patient's health care has both pros and cons. On the one hand, a patient may benefit from being referred to specialists with more expertise in treating the patient's medical conditions. On the other hand, as more providers are involved in care, the primary care provider may find it more difficult to coordinate among providers. Weak coordination makes it harder to clarify responsibilities for ongoing care, and to avoid redundant and unnecessary care.
Care fragmentation occurs when the delivery of health care is spread across an excessively large number of poorly coordinated providers. Care fragmentation is considered to be a potentially important source of inefficiency in the U.S. health care system, yet its causes and consequences are not well understood.
Researchers Leila Agha, Brigham Frandsen, and James Rebitzer explore this issue in their new working paper, Causes and Consequences of Fragmented Care Delivery: Theory, Evidence, and Public Policy (NBER Working Paper No. 23078).
The researchers begin by building a model of health care fragmentation in which primary care providers balance the benefits to the patient of specialist care against the costs of more difficult care coordination. Getting this balance right is complicated by the presence of spillover effects: physicians who refer more to specialists get better at coordinating among specialists, while those who refer less get better at providing direct care to patients. These spillover effects cause regional differences in practice styles such that a patient who receives highly fragmented care in one region could experience much less fragmentation of care if they moved to another region.
In their empirical study of fragmentation, the researchers use Medicare claims data to construct a measure of how concentrated patient visits are across their various providers. An advantage of this measure over a simple count of providers is that a patient who gets most of her care from one or a few providers will have a low fragmentation score, even if she has seen many other providers in a limited way, such as for a single visit.
Using this measure, the researchers find that there are substantial regional differences in fragmentation and that these are strongly associated with differences in resource utilization. Consistent with their model of spillover effects, they also find that Medicare enrollees who move across regions find that the degree of care fragmentation they experience shifts strongly and immediately toward the style of care prevalent in their new region.
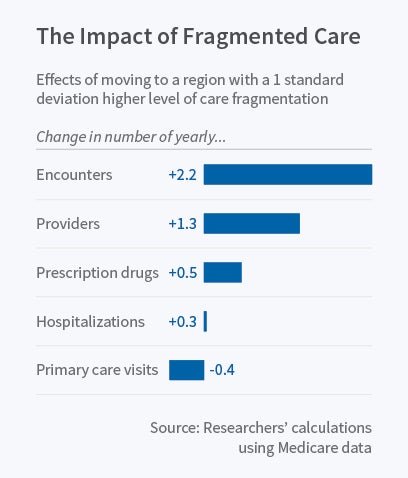
The researchers estimate that moving to a region with a one standard deviation higher level of regional fragmentation is also associated with a 10 percent increase in care utilization. Moves toward more fragmented regions are also associated with an increase in provider visits, fewer visits with primary care providers, and greater reliance on specialists whose scope of practice overlaps with primary care providers. The reverse happens when Medicare enrollees move to less fragmented regions. These findings suggest that "in more fragmented regions, specialists take on the management of conditions that could otherwise be treated by primary care providers."
In more fine-grained analyses, the researchers report that moving to regions where patient care is divided across many pri-mary care providers markedly increases hospitalizations, suggesting that a consistent relationship with a primary care provider may reduce demand for hospital care. One explanation for this result is that primary care fragmentation causes deterioration in patients' health; alternatively, regions with fragmented primary care may rely more heavily on hospitalization for a given disease state. This association stands in contrast to the effect of moving to a region that makes heavier use of different types of specialist physicians; fragmentation of care driven by specialist use is not associated with greater use of hospitalization.
In the public policy realm, recent anti-fragmentation initiatives, such as Accountable Care Organizations, aim to reduce costly fragmentation by altering provider financial incentives. The spillover effects that cause regional differences in fragmentation patterns, however, complicate any analysis of the effects of these incentives. Using their theoretical model of care fragmentation, the researchers do find that better incentives may improve the delivery of health care — but only when fragmented care is also more costly. The paper concludes that "much more remains to be learned about effective public policy responses to fragmented care delivery."


