Examining an Aging Population in Sub-Saharan Africa
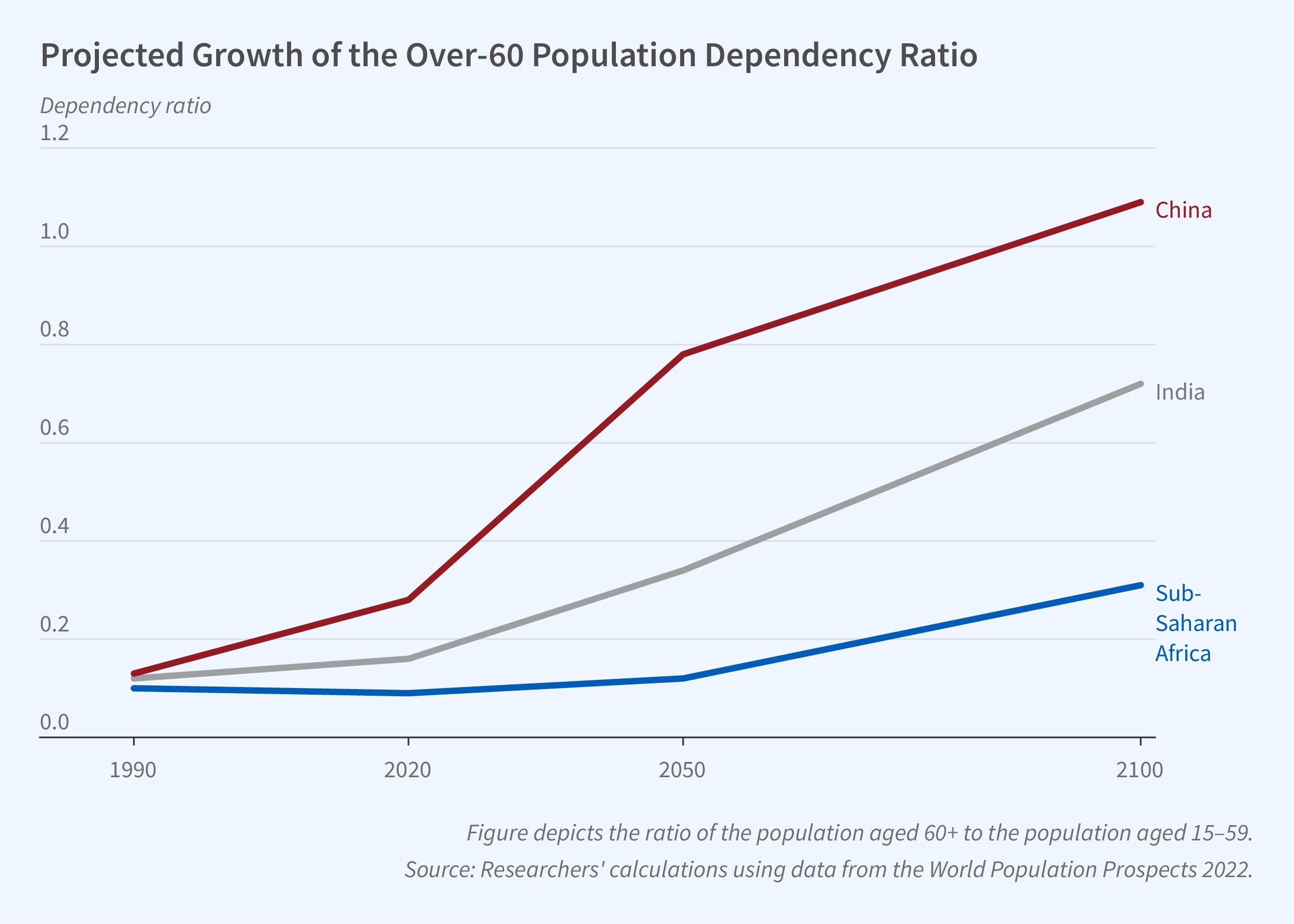
In Preparing for an Aging Africa: Data-Driven Priorities for Economic Research and Policy (NBER Working Paper 31750), researchers Madeline E. Duhon, Edward Miguel, Amos Njuguna, Daniela Pinto Veizaga, and Michael W. Walker review previous literature and conduct new analysis drawing on 35 rounds of nationally representative household survey data from 8 countries to identify challenges facing Sub-Saharan Africa due to its aging population. The UN World Population Prospects projects the over-60 population in Sub-Saharan Africa will increase from 50 million in 2020 to 600 million by 2100. This represents a shift in demographic composition, with individuals above age 60 constituting 5 percent of the population in 2020 and nearly 20 percent by 2100. Consequently, the old-age dependency ratio, the proportion of individuals aged 60+ to those aged 15–59, will increase by the century’s end.
In Sub-Saharan Africa, the proportion of elderly individuals relative to the working-age population is expected to increase throughout the remainder of the 21st century.
The researchers highlight that Sub-Saharan Africa currently lags in healthcare and public support systems compared to other low- or middle-income countries (LMICs) and high-income countries (HICs). The region’s governments spend a smaller share of GDP on health, leading to fewer hospital beds and medical professionals per capita. Approximately 80 percent of health budgets are allocated to infectious diseases, with little spending on non communicable conditions, which disproportionately affect the elderly. They highlight that — according to data from the International Labor Organization (ILO) — only about one percent of GDP is spent on pensions and other social programs for older individuals, compared to an average of 4 percent in other LMICs and 8 percent in HICs, respectively.
Many older individuals face locational, financial, and non financial barriers to accessing healthcare. The researchers document that the elderly are more likely to reside in rural areas, where healthcare centers may be more remote or of lower quality. In Nigeria, Kenya, and Uganda, the elderly are more likely to report that they lack access to healthcare facilities and are less likely to seek care compared to other age groups. Regionwide, only 8 percent of the elderly benefit from health insurance.
Functional limitations are prevalent among the elderly in the region, with the share of individuals reporting limitations rising from about 25 percent at age 60 to over 50 percent at ages 80 and above. About 30 percent of the elderly population reports experiencing a recent illness or injury that required them to stop work or their usual activities. Alzheimer’s disease and related dementias — conditions that are potentially stigmatized and underdiagnosed in this context — are of particular concern, with the number of persons living with these conditions expected to triple from 2.1 million in 2015 to 7.5 million in 2050, according to previous research.
Another area of concern is mental health, with depression prevalence increasing with age. The researchers estimate, for instance, that in Ghana 28 percent of those over 80 experienced moderate or severe psychological distress, compared to 13 percent of those aged 20–60. However, spending on mental health in Africa is low, with government expenditure per capita being less than $0.50 in 2020, compared to over $50 in HICs, as reported by the World Health Organization.
Pension receipt is far from universal, with less than a quarter of the elderly in Sub-Saharan Africa receiving any pension. In the absence of public support, elderly individuals often rely on family-based caregiving. In Nigeria, over two-thirds are cared for by children or children-in-law, mainly daughters and daughters-in-law. These forms of care may come under strain due to rural-urban migration, industrialization, and shifting social norms. Falling fertility rates, increasing female labor force participation rates, and rural-urban migration have all led to a decrease in the number of available caregivers. Conditions for older individuals in the region in the future could be complicated by the impacts of climate change as well as other economic, political, and social developments.
On the other hand, most African countries are projected to experience positive economic growth, as well as substantial growth in the working-age population, which can increase household resources and provide additional funding for public programs. In contrast to regions like Europe and East Asia that have declining working-age populations, Sub-Saharan Africa may be poised to reap the benefits of a demographic dividend. More aging-focused research in Sub-Saharan Africa can shed light on the needs of its aging population and inform the design of effective policies.
— Leonardo Vasquez
The research reported herein was performed pursuant to grant RDR18000003 from the US Social Security Administration (SSA) funded as part of the Retirement and Disability Research Consortium. The opinions and conclusions expressed are solely those of the author(s) and do not represent the opinions or policy of SSA, any agency of the federal government, or NBER. Neither the United States Government nor any agency thereof, nor any of their employees, makes any warranty, express or implied, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of the contents of this report. Reference herein to any specific commercial product, process or service by trade name, trademark, manufacturer, or otherwise does not necessarily constitute or imply endorsement, recommendation or favoring by the United States Government or any agency thereof. The researchers gratefully acknowledge funding from the National Institute on Aging of the National Institutes of Health (NIH) under award number R01AG077001; as well as funding and support from a training grant awarded to UC Berkeley (NIH T32AG000246), the UC Berkeley Demography Department, and the Berkeley Population Center. The views expressed herein are those of the authors and do not necessarily reflect the views of the National Bureau of Economic Research.


